Home /
Second Degree AV block - Conduction 2:1
2:1 2nd degree AV block, Fixed-Ratio 2:1 AV block
Atrioventricular (AV) Node

- In sinus rhythm, impulses are generated regularly (approx. 60/min) in the SA node
- Each impulse spreads through the atria (P wave) to the AV node
- The impulse slows down in the AV node by about 0.1s
- During this time, the atria pump blood into the ventricles
- Then the impulse continues to the ventricles (QRS complex)
PQ Interval

- An impulse originates in the SA node
- As it passes to the atrial myocardium, the P wave begins to form
- Simultaneously, it spreads through the conduction system towards the AV node
- The impulse in the conduction system does not create a wave
- The impulse enters the AV node
- The impulse spreads from the SA node
- At the time of atrial activation (peak of the P wave)
- It reaches the AV node through the conduction system
- Slowed (decremental) conduction of the AV node
- The impulse delays in the AV node for approx. 0.1s (no wave is formed)
- Then it passes into the His bundle (no wave is formed)
- Activation of the ventricular septum
- From the His bundle, the impulse travels through the Purkinje fibers
- It begins to activate the myocardium of the ventricular septum
- The Q wave starts to form
AV Block II Degree (Mobitz I, Mobitz II)
- Woldemar Mobitz
- Was a Russian doctor who worked as a cardiologist in Germany
- In 1924, he described AV block II degree on an ECG and divided it into 2 types (Mobitz I, II)
- Mobitz I (Wenckebach)
- Often referred to as Wenckebach
- Because there is a Wenckebach phenomenon in the AV node
- Mobitz II (Hay)
- John Hay was an English doctor who described this AV block II degree based on pulses (without ECG) in 1906
- It was later detailed by Mobitz and is more commonly referred to as Mobitz II, rarely as Hay
AV Block II Degree - Mobitz I (Wenckebach)
- Mobitz I is a nodal disorder (disorder in the AV node)
- Impulse conduction through the AV node gradually prolongs until the impulse is blocked (Wenckebach phenomenon)
- The ventricles are activated through the conduction system (His bundle, bundle branches...)
- Therefore, the QRS complexes are narrow (<0.12s)

AV Block II Degree - Mobitz I (Wenckebach)
- Laddergram illustrates the spread of the impulse through the conduction system
- A - Atria, AV - AV junction, V - Ventricles
- Mobitz I is a disorder of the AV node (which has the Wenckebach phenomenon)
- PP interval is constant (810ms) - sinus rhythm
- QRS complexes are narrow (<0.12s)
- PQ interval gradually prolongs until the P wave is blocked (no QRS complex follows the P wave)
- 1st PQ (190ms)
- 2nd PQ (290ms)
- 3rd P wave is blocked
- The cycle then repeats
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree - Mobitz II (QRS<0.12s)
- Mobitz II is an infranodal disorder (somewhere below the AV node)
- 25% of Mobitz II AV blocks have a narrow QRS complex (<0.12s), if aberrant conduction is not present
- The disorder is located in the His bundle
- Intermittent blockage of impulses occurs in the His bundle
- Unblocked impulses are conducted to the ventricles through the conduction system
- Therefore, the QRS complexes are narrow (<0.12s)
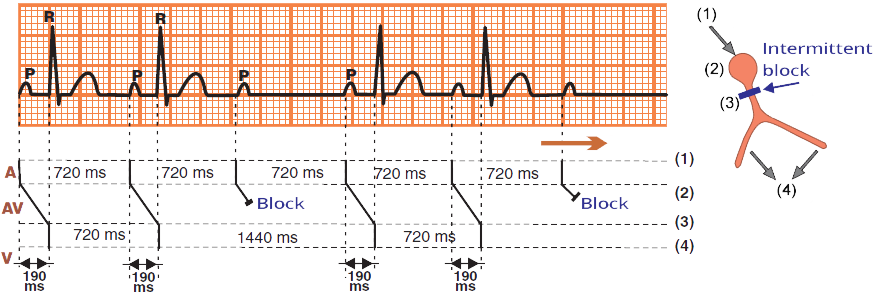
AV Block II Degree - Mobitz II
- Mobitz II is an infranodal disorder (below the AV node)
- PP interval is constantly the same (720ms)
- Narrow QRS complexes (<0.12s)
- PQ interval is constantly the same (190ms), this is the main difference from Mobitz I (Wenckebach)
- Every 3rd P wave is blocked in the His bundle
- No QRS complex follows it
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree - Mobitz II (QRS>0.12s)
- 75% of Mobitz II AV blocks have a wide QRS complex (>0.12s)
- Because it is an infrahisian block (below the His bundle)
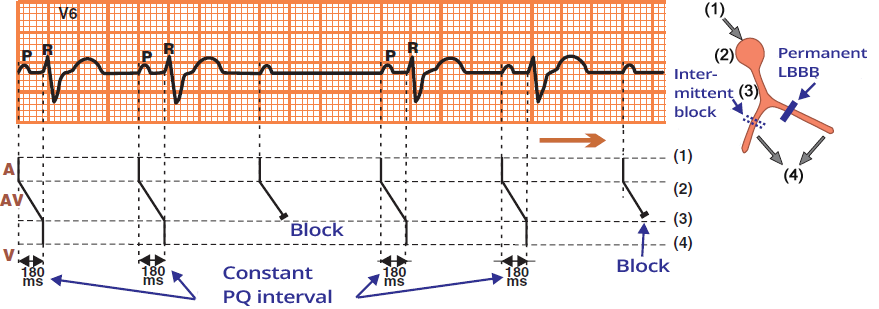
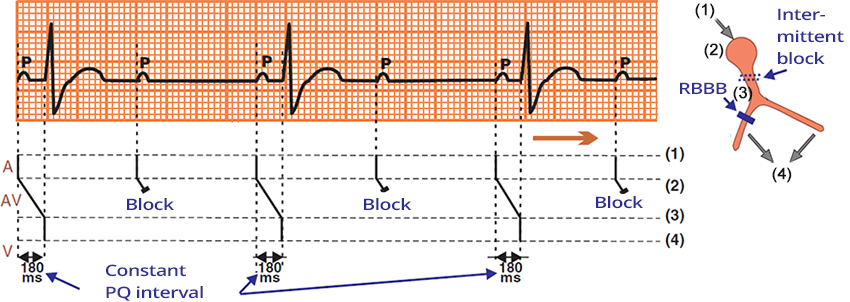
AV Block II Degree - Mobitz II
- This is an infrahisian AV block II degree - Mobitz II
- 75% of Mobitz II AV blocks have a wide QRS complex (>0.12s)
- Mobitz II can block impulses infrahisially: at the level of the bundle branches or fascicles
- The likelihood of having an intermittent block at
- 2 sites (2 bundle branches)
- 3 sites (2 fascicles and the right bundle branch)
- is minimal
- Patients have a wide QRS complex because they have a pre-existing:
- In sinus rhythm, impulses pass to the ventricles through only one intact bundle branch (fascicle)
- On the ECG, there is a wide QRS complex
- Intermittent blockage of impulses occurs in the unblocked bundle branch (fascicle)
- Which we see on the ECG as blocked P waves (no QRS complex follows)
- PQ interval is constantly the same (180ms), this is the main difference from Mobitz I (Wenckebach)
- Every 3rd P wave is blocked below the His bundle
- No QRS complex follows it
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree with Conduction (2:1)

AV Block II Degree with Conduction (2:1)
- Conduction to the ventricles is 2:1 (every second P wave is blocked - blue arrows)
- With 2:1 conduction, it is questionable whether it is Mobitz I or Mobitz II?
- We don't know if the PQ interval is lengthening (Mobitz I), or if every second P wave is blocked (Mobitz II)
Differential Diagnosis - AV Block II Degree (2:1)
- Have the patient undergo a long ECG recording
- On a long ECG recording, another conduction to the ventricles other than (2:1) will sooner or later appear
- AV Block II Degree - Mobitz I (Nodal disorder)
- Forms narrow QRS complexes because the impulse passes to the ventricles through the AV junction and through the conduction system
- In the AV node, there is a Wenckebach phenomenon (PQ interval gradually lengthens until the P wave is not conducted)
- AV Block II Degree - Mobitz II (Infranodal disorder)
- 75% of Mobitz II forms wide QRS (Infrahisian disorder)
- The patient already has a pre-existing bundle branch block (LBBB, RBBB), or a Bifascicular block
- Therefore, the QRS complexes are wide
- 25% of Mobitz II forms narrow QRS (Hisian disorder)
- The conduction system, except for the His bundle, is intact
- PQ interval in AV block II degree (2:1)
- Mobitz I has a prolonged PQ interval (almost always, but not a rule)
- Mobitz II has a non-prolonged PQ interval
- Administration of atropine in AV block II degree (2:1)
- Atropine is a parasympatholytic, it increases the frequency of the SA node and accelerates conduction through the AV node
- Mobitz I improves
- It is a disorder of the AV node and atropine acts on the AV node
- Conduction through the AV node increases, Wenckebach phenomenon subsides
- A block (2:1) becomes a milder block (3:2, 4:3, 5:4)
- Mobitz II worsens
- It is an infranodal disorder, not an AV node disorder, and atropine acts on the AV node
- Mobitz II (2:1) may not respond to atropine, the conduction to the ventricles remains (2:1)
- After atropine, the frequency of the SA node increases and the conduction system below the AV junction is frequency overloaded
- Carotid sinus massage in AV block II degree (2:1)
- Carotid sinus massage blocks the AV node (slows conduction through the AV node) and reduces the frequency of the SA node
- Mobitz I worsens
- It is a disorder of the AV node and carotid sinus massage blocks the AV node
- A block (2:1) becomes a worse block (3:1, 4:1, 5:1)
- Mobitz II improves
- It is an infranodal disorder, not an AV node disorder, and carotid sinus massage blocks the AV node
- The frequency of the SA node decreases and conduction through the AV node lengthens
- The conduction system below the AV node (where the Mobitz II disorder is)
- is less burdened due to the lower frequency
- Therefore, Mobitz II may improve, a block (2:1) becomes (3:2, 4:3, 5:4)

AV Block II Degree with Conduction (2:1)

AV Block II Degree with Conduction (2:1)
- Every second P wave is blocked (blue arrows)
- Narrow QRS complexes (< 0.12s)
- which suggests Mobitz I, very rarely Mobitz II
- Non-prolonged PQ interval (< 0.2s)
- suggests more likely Mobitz II
- Most likely it is AV Block II Degree - Mobitz I (narrow QRS complexes)

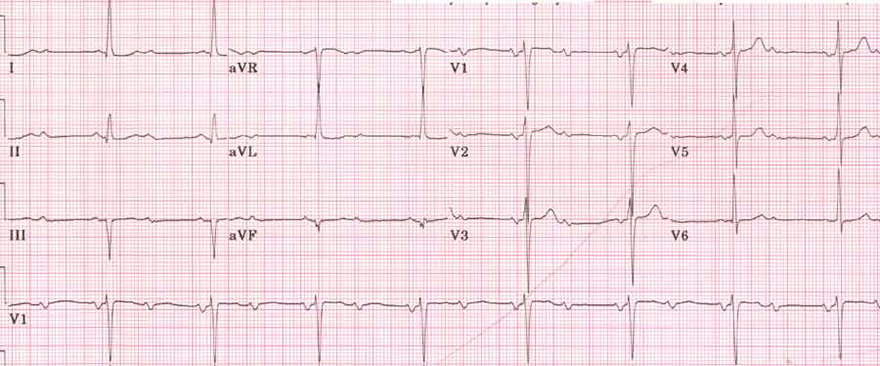
AV Block II Degree with Conduction (2:1)
- Narrow QRS complexes (< 0.12s)
- which suggests Mobitz I, very rarely Mobitz II
- Prolonged PQ interval (> 0.2s)
- Most likely it is AV Block II Degree - Mobitz I
- the patient later had a long EKG recording

AV Block II Degree - Mobitz I (Wenckebach)
- This is a longer EKG recording from the passing patient
- Note the 5th and 6th QRS complexes
- The PQ interval is progressively prolonged until a P wave is blocked, without a QRS (the blocked P wave is hidden in the T wave)
- This is AV Block II Degree - Mobitz I (Wenckebach) (because the PQ interval is prolonged)
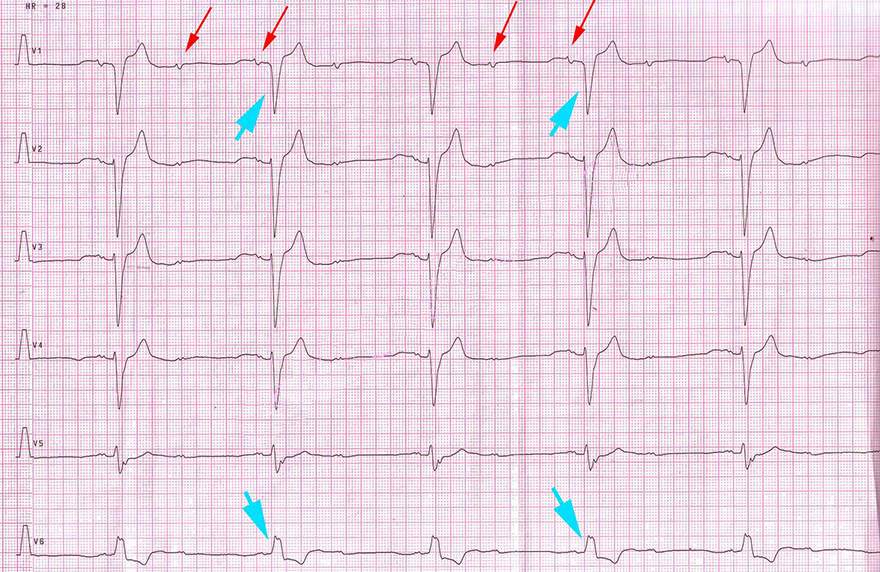
AV Block II Degree with Conduction (2:1)
- Wide QRS complexes (> 0.12s), suggests Mobitz II
- Non-prolonged PQ interval (< 0.2s), more indicative of Mobitz II
- According to the laddergram, it is Hisian AV Block II Degree - Mobitz II
AV Block II Degree with Conduction (2:1)
AV Block II Degree with Conduction (2:1)
- Narrow QRS complexes (< 0.12s)
- Suggestive of Mobitz I, very rarely Mobitz II
- Non-prolonged PQ interval (< 0.2s)
- More indicative of Mobitz II
- Most likely AV Block II Degree - Mobitz I (narrow QRS complexes)
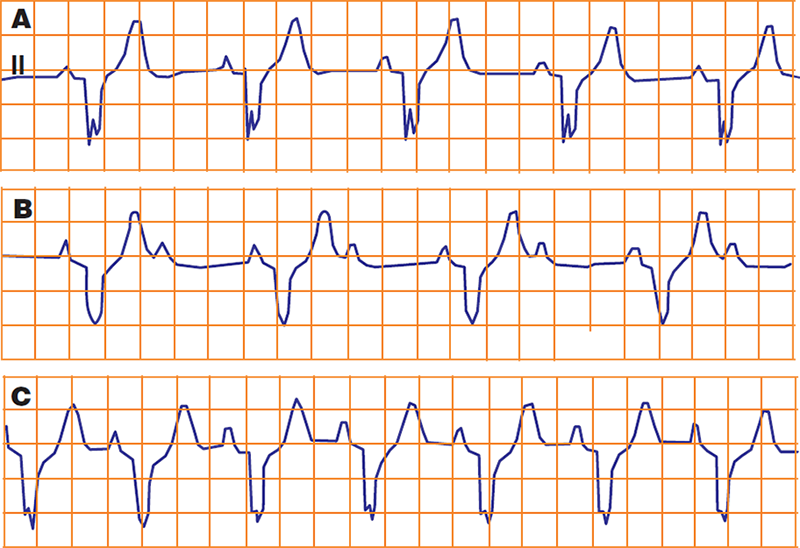
AV Block II Degree with Conduction (2:1)
- This is a continuous EKG recording (Lead II), which was taken during ergometry
- A - Resting EKG
- B - EKG during ergometry:
- During exercise, the rate increased to 110/min. (P wave frequency)
- There was a functional AV block II degree with 2:1 conduction
- Due to ischemic damage to the AV junction (during tachycardia)
- C - The patient stopped cycling
- The rate began to decrease to 80/min., and the AV block (2:1) resolved
- AV blocks during exertion occur due to infranodal AV block (Mobitz II)
Sources
- ECG from Basics to Essentials Step by Step
- litfl.com
- ecgwaves.com
- metealpaslan.com
- medmastery.com
- uptodate.com
- ecgpedia.org
- wikipedia.org
- Strong Medicine
- Understanding Pacemakers

Home /
Second Degree AV block - Conduction 2:1
2:1 2nd degree AV block, Fixed-Ratio 2:1 AV block
Atrioventricular (AV) Node
- In sinus rhythm, impulses are generated regularly (approx. 60/min) in the SA node
- Each impulse spreads through the atria (P wave) to the AV node
- The impulse slows down in the AV node by about 0.1s
- During this time, the atria pump blood into the ventricles
- Then the impulse continues to the ventricles (QRS complex)
|
|
PQ Interval
- An impulse originates in the SA node
- As it passes to the atrial myocardium, the P wave begins to form
- Simultaneously, it spreads through the conduction system towards the AV node
- The impulse in the conduction system does not create a wave
- The impulse enters the AV node
- The impulse spreads from the SA node
- At the time of atrial activation (peak of the P wave)
- It reaches the AV node through the conduction system
- Slowed (decremental) conduction of the AV node
- The impulse delays in the AV node for approx. 0.1s (no wave is formed)
- Then it passes into the His bundle (no wave is formed)
- Activation of the ventricular septum
- From the His bundle, the impulse travels through the Purkinje fibers
- It begins to activate the myocardium of the ventricular septum
- The Q wave starts to form
|
|
AV Block II Degree (Mobitz I, Mobitz II)
- Woldemar Mobitz
- Was a Russian doctor who worked as a cardiologist in Germany
- In 1924, he described AV block II degree on an ECG and divided it into 2 types (Mobitz I, II)
- Mobitz I (Wenckebach)
- Often referred to as Wenckebach
- Because there is a Wenckebach phenomenon in the AV node
- Mobitz II (Hay)
- John Hay was an English doctor who described this AV block II degree based on pulses (without ECG) in 1906
- It was later detailed by Mobitz and is more commonly referred to as Mobitz II, rarely as Hay
AV Block II Degree - Mobitz I (Wenckebach)
- Mobitz I is a nodal disorder (disorder in the AV node)
- Impulse conduction through the AV node gradually prolongs until the impulse is blocked (Wenckebach phenomenon)
- The ventricles are activated through the conduction system (His bundle, bundle branches...)
- Therefore, the QRS complexes are narrow (<0.12s)
AV Block II Degree - Mobitz I (Wenckebach)
- Laddergram illustrates the spread of the impulse through the conduction system
- A - Atria, AV - AV junction, V - Ventricles
- Mobitz I is a disorder of the AV node (which has the Wenckebach phenomenon)
- PP interval is constant (810ms) - sinus rhythm
- QRS complexes are narrow (<0.12s)
- PQ interval gradually prolongs until the P wave is blocked (no QRS complex follows the P wave)
- 1st PQ (190ms)
- 2nd PQ (290ms)
- 3rd P wave is blocked
- The cycle then repeats
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree - Mobitz II (QRS<0.12s)
- Mobitz II is an infranodal disorder (somewhere below the AV node)
- 25% of Mobitz II AV blocks have a narrow QRS complex (<0.12s), if aberrant conduction is not present
- The disorder is located in the His bundle
- Intermittent blockage of impulses occurs in the His bundle
- Unblocked impulses are conducted to the ventricles through the conduction system
- Therefore, the QRS complexes are narrow (<0.12s)
AV Block II Degree - Mobitz II
- Mobitz II is an infranodal disorder (below the AV node)
- PP interval is constantly the same (720ms)
- Narrow QRS complexes (<0.12s)
- PQ interval is constantly the same (190ms), this is the main difference from Mobitz I (Wenckebach)
- Every 3rd P wave is blocked in the His bundle
- No QRS complex follows it
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree - Mobitz II (QRS>0.12s)
- 75% of Mobitz II AV blocks have a wide QRS complex (>0.12s)
- Because it is an infrahisian block (below the His bundle)
AV Block II Degree - Mobitz II
- This is an infrahisian AV block II degree - Mobitz II
- 75% of Mobitz II AV blocks have a wide QRS complex (>0.12s)
- Mobitz II can block impulses infrahisially: at the level of the bundle branches or fascicles
- The likelihood of having an intermittent block at
- 2 sites (2 bundle branches)
- 3 sites (2 fascicles and the right bundle branch)
- is minimal
- Patients have a wide QRS complex because they have a pre-existing:
- In sinus rhythm, impulses pass to the ventricles through only one intact bundle branch (fascicle)
- On the ECG, there is a wide QRS complex
- Intermittent blockage of impulses occurs in the unblocked bundle branch (fascicle)
- Which we see on the ECG as blocked P waves (no QRS complex follows)
- PQ interval is constantly the same (180ms), this is the main difference from Mobitz I (Wenckebach)
- Every 3rd P wave is blocked below the His bundle
- No QRS complex follows it
- Conduction to the ventricles is (3:2)
- Of 3 P waves, 2 P waves are conducted to the ventricles (2 QRS complexes are produced), the cycle then repeats
AV Block II Degree with Conduction (2:1)
AV Block II Degree with Conduction (2:1)
- Conduction to the ventricles is 2:1 (every second P wave is blocked - blue arrows)
- With 2:1 conduction, it is questionable whether it is Mobitz I or Mobitz II?
- We don't know if the PQ interval is lengthening (Mobitz I), or if every second P wave is blocked (Mobitz II)
Differential Diagnosis - AV Block II Degree (2:1)
- Have the patient undergo a long ECG recording
- On a long ECG recording, another conduction to the ventricles other than (2:1) will sooner or later appear
- AV Block II Degree - Mobitz I (Nodal disorder)
- Forms narrow QRS complexes because the impulse passes to the ventricles through the AV junction and through the conduction system
- In the AV node, there is a Wenckebach phenomenon (PQ interval gradually lengthens until the P wave is not conducted)
- AV Block II Degree - Mobitz II (Infranodal disorder)
- 75% of Mobitz II forms wide QRS (Infrahisian disorder)
- The patient already has a pre-existing bundle branch block (LBBB, RBBB), or a Bifascicular block
- Therefore, the QRS complexes are wide
- 25% of Mobitz II forms narrow QRS (Hisian disorder)
- The conduction system, except for the His bundle, is intact
- PQ interval in AV block II degree (2:1)
- Mobitz I has a prolonged PQ interval (almost always, but not a rule)
- Mobitz II has a non-prolonged PQ interval
- Administration of atropine in AV block II degree (2:1)
- Atropine is a parasympatholytic, it increases the frequency of the SA node and accelerates conduction through the AV node
- Mobitz I improves
- It is a disorder of the AV node and atropine acts on the AV node
- Conduction through the AV node increases, Wenckebach phenomenon subsides
- A block (2:1) becomes a milder block (3:2, 4:3, 5:4)
- Mobitz II worsens
- It is an infranodal disorder, not an AV node disorder, and atropine acts on the AV node
- Mobitz II (2:1) may not respond to atropine, the conduction to the ventricles remains (2:1)
- After atropine, the frequency of the SA node increases and the conduction system below the AV junction is frequency overloaded
- Carotid sinus massage in AV block II degree (2:1)
- Carotid sinus massage blocks the AV node (slows conduction through the AV node) and reduces the frequency of the SA node
- Mobitz I worsens
- It is a disorder of the AV node and carotid sinus massage blocks the AV node
- A block (2:1) becomes a worse block (3:1, 4:1, 5:1)
- Mobitz II improves
- It is an infranodal disorder, not an AV node disorder, and carotid sinus massage blocks the AV node
- The frequency of the SA node decreases and conduction through the AV node lengthens
- The conduction system below the AV node (where the Mobitz II disorder is)
- is less burdened due to the lower frequency
- Therefore, Mobitz II may improve, a block (2:1) becomes (3:2, 4:3, 5:4)
AV Block II Degree with Conduction (2:1)
AV Block II Degree with Conduction (2:1)
- Every second P wave is blocked (blue arrows)
- Narrow QRS complexes (< 0.12s)
- which suggests Mobitz I, very rarely Mobitz II
- Non-prolonged PQ interval (< 0.2s)
- suggests more likely Mobitz II
- Most likely it is AV Block II Degree - Mobitz I (narrow QRS complexes)
AV Block II Degree with Conduction (2:1)
- Narrow QRS complexes (< 0.12s)
- which suggests Mobitz I, very rarely Mobitz II
- Prolonged PQ interval (> 0.2s)
- Most likely it is AV Block II Degree - Mobitz I
- the patient later had a long EKG recording
AV Block II Degree - Mobitz I (Wenckebach)
- This is a longer EKG recording from the passing patient
- Note the 5th and 6th QRS complexes
- The PQ interval is progressively prolonged until a P wave is blocked, without a QRS (the blocked P wave is hidden in the T wave)
- This is AV Block II Degree - Mobitz I (Wenckebach) (because the PQ interval is prolonged)
AV Block II Degree with Conduction (2:1)
- Wide QRS complexes (> 0.12s), suggests Mobitz II
- Non-prolonged PQ interval (< 0.2s), more indicative of Mobitz II
- According to the laddergram, it is Hisian AV Block II Degree - Mobitz II
AV Block II Degree with Conduction (2:1)
AV Block II Degree with Conduction (2:1)
- Narrow QRS complexes (< 0.12s)
- Suggestive of Mobitz I, very rarely Mobitz II
- Non-prolonged PQ interval (< 0.2s)
- More indicative of Mobitz II
- Most likely AV Block II Degree - Mobitz I (narrow QRS complexes)
AV Block II Degree with Conduction (2:1)
- This is a continuous EKG recording (Lead II), which was taken during ergometry
- A - Resting EKG
- B - EKG during ergometry:
- During exercise, the rate increased to 110/min. (P wave frequency)
- There was a functional AV block II degree with 2:1 conduction
- Due to ischemic damage to the AV junction (during tachycardia)
- C - The patient stopped cycling
- The rate began to decrease to 80/min., and the AV block (2:1) resolved
- AV blocks during exertion occur due to infranodal AV block (Mobitz II)
Sources
- ECG from Basics to Essentials Step by Step
- litfl.com
- ecgwaves.com
- metealpaslan.com
- medmastery.com
- uptodate.com
- ecgpedia.org
- wikipedia.org
- Strong Medicine
- Understanding Pacemakers