|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |


Myocardial Depolarization


Myocardial Repolarization

Physiological T Wave
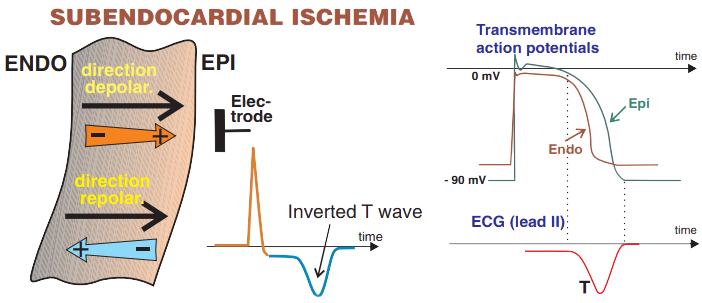
Subendocardial Ischemia
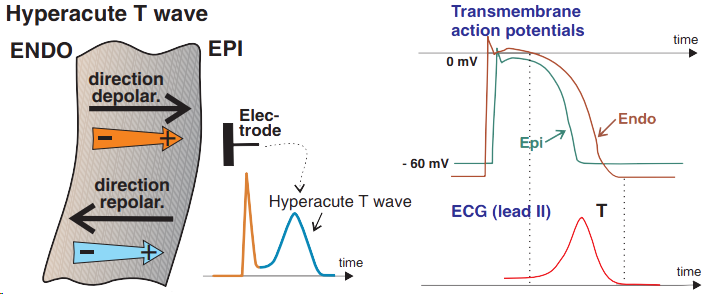
Subepicardial and Transmural Ischemia
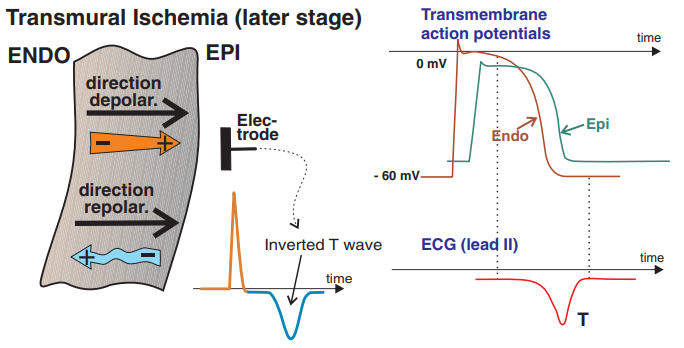
Late Transmural Ischemia

Unstable Angina Pectoris

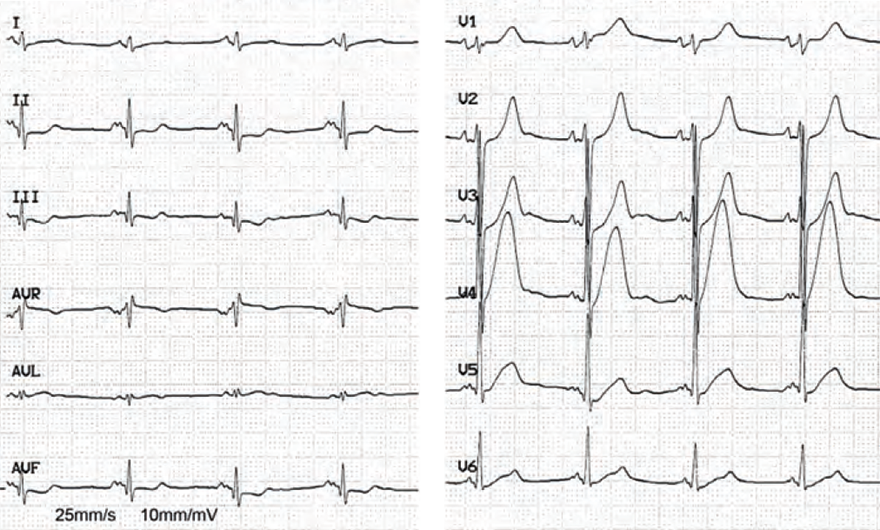
Hyperacute STEMI of the Anterior Wall

Old Anterior STEMI
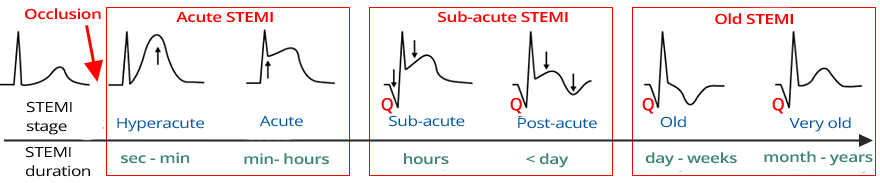
STEMI Classification by Stage
Sources
|
|
Myocardial Depolarization
|
|
|
Myocardial Repolarization
|
Physiological T Wave
Subendocardial Ischemia
Subepicardial and Transmural Ischemia
Late Transmural Ischemia
|
Unstable Angina Pectoris
|
|
|
Hyperacute STEMI of the Anterior Wall
|
|
|
Old Anterior STEMI
|
|
STEMI Classification by Stage
Sources