|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
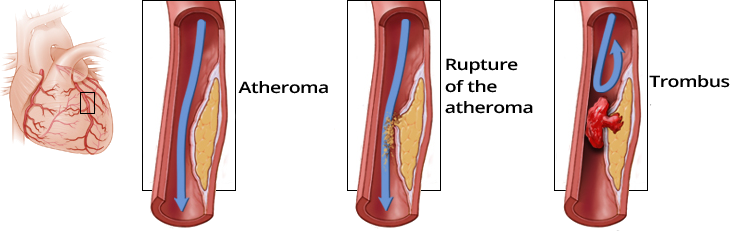
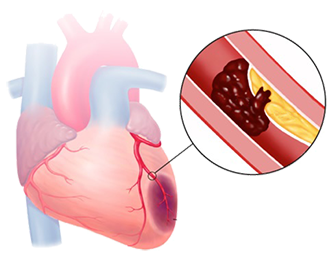
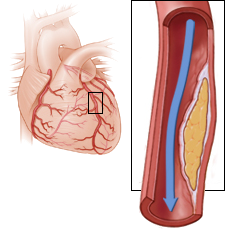
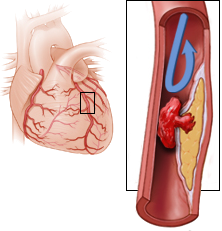
Atherosclerosis and Acute Coronary Syndrome
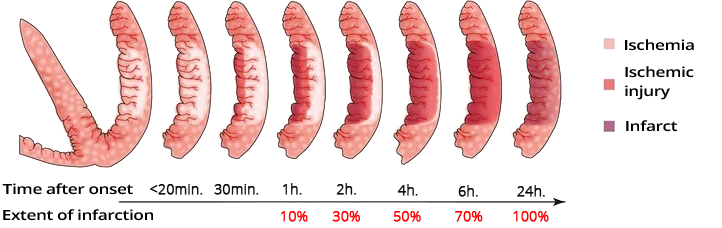
Dynamics of Ischemia after Occlusion
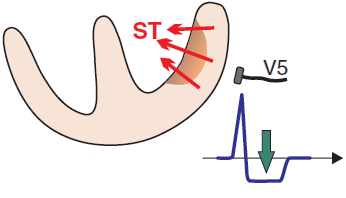
ST Segment and Acute Coronary Syndrome
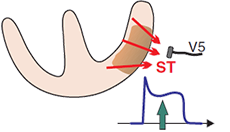
Subendocardial Ischemia

Subepicardial Ischemia
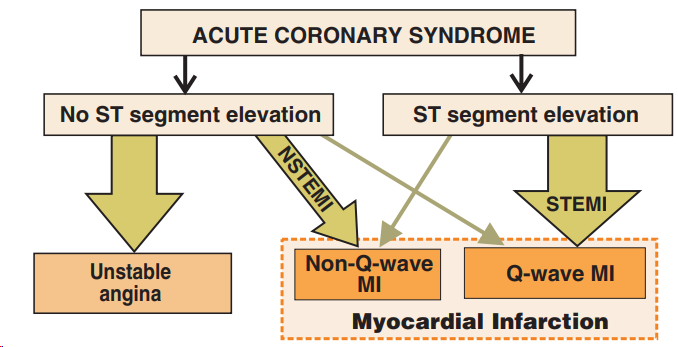
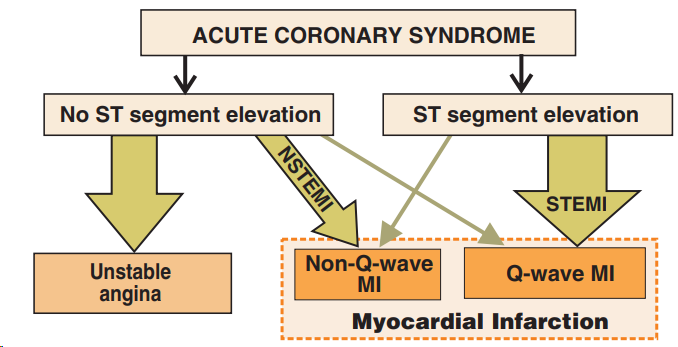
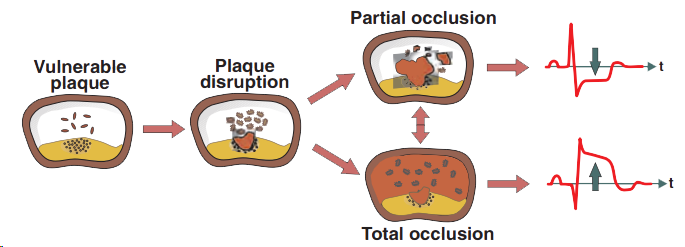
Acute Coronary Syndrome
STEMI Infarction

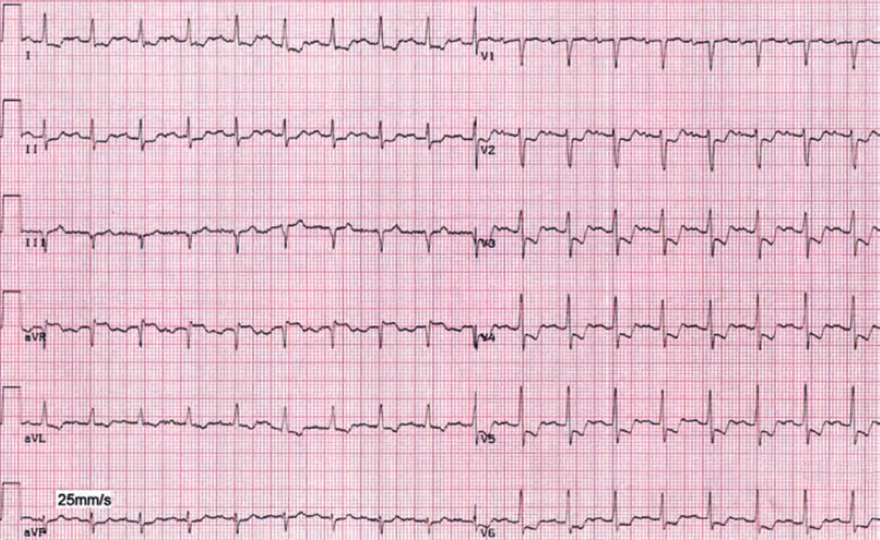
NSTEMI Infarction
Ischemia Post-Ergometry

Unstable Angina Pectoris
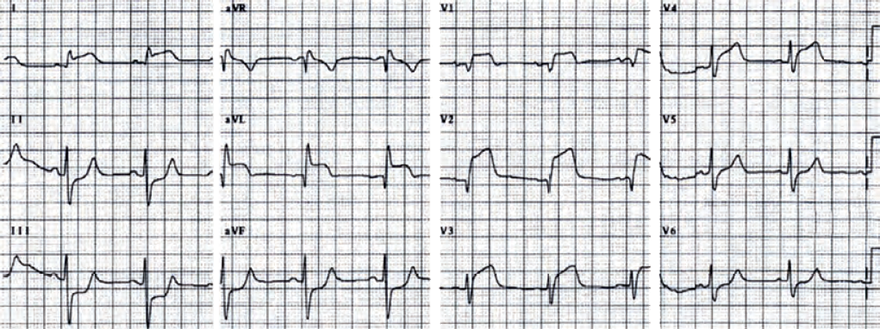
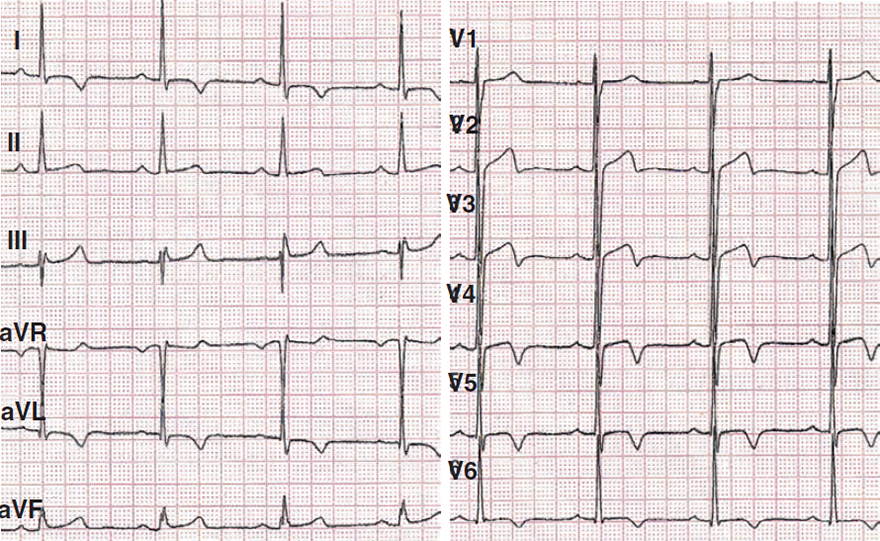
Acute STEMI of the Anterior Wall
Sources
Atherosclerosis and Acute Coronary Syndrome
Dynamics of Ischemia in Occlusion
|
|
Dynamics of Ischemia after Occlusion
ST Segment and Acute Coronary Syndrome
|
Subendocardial Ischemia
|
Subepicardial Ischemia
|
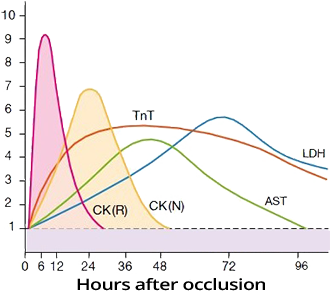
Troponin and Infarction
|
|
Acute Coronary Syndrome (ACS)
|
|
Acute Coronary Syndrome
Nomenclature of Infarction
|
STEMI Infarction
|
NSTEMI Infarction
|
|
Ischemia Post-Ergometry
|
|
|
Unstable Angina Pectoris
|
|
|
Acute STEMI of the Anterior Wall
|
|
Sources