|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
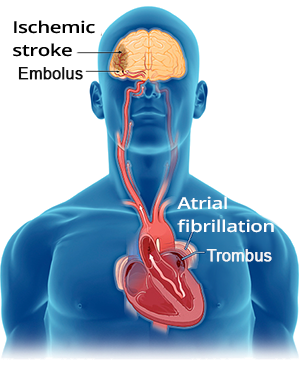


Atrial Fibrillation
Atrial Fibrillation and Frequency 130/min.
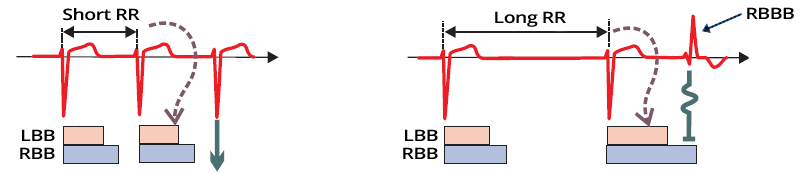

Ashman Phenomenon and Atrial Fibrillation

Atrial Fibrillation

Atrial Flutter with Variable Conduction (2:1 and 4:1)


Multifocal Atrial Tachycardia
Atrial Fibrillation
Atrial Flutter (with Variable Conduction 2:1 and 4:1)
Atrial Fibrillation
Atrial Fibrillation
Multifocal Atrial Tachycardia
Atrial Fibrillation
Atrial Fibrillation
Atrial Fibrillation and Ashman’s Phenomenon
Atrial Fibrillation and Ashman’s Phenomenon
Sources
|
|
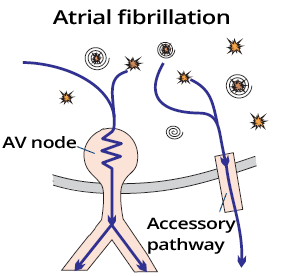
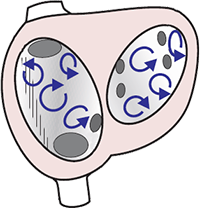
Atria and Atrial Fibrillation
|
|
|
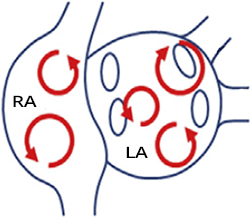
Numerous Micro Re-entries
|
|
|
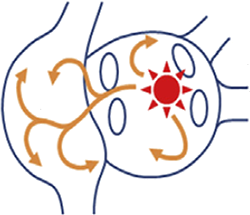
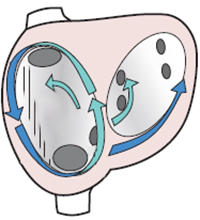
Focal Focus and Activation Waves
|
|
|
Maternal Re-entry and Activation Waves
|
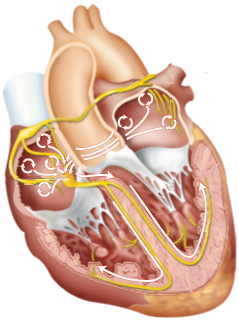
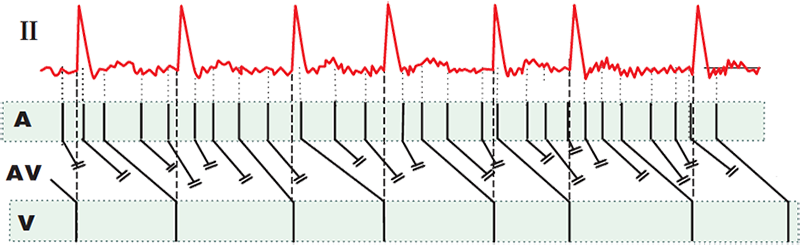
Protective Mechanism of the AV Node
|
|
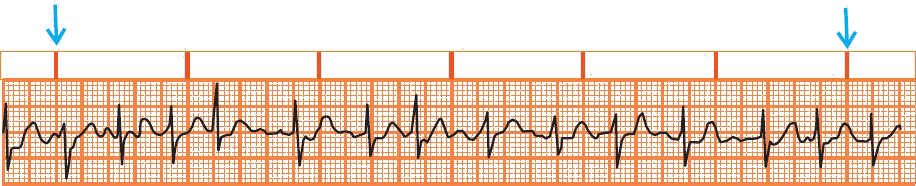
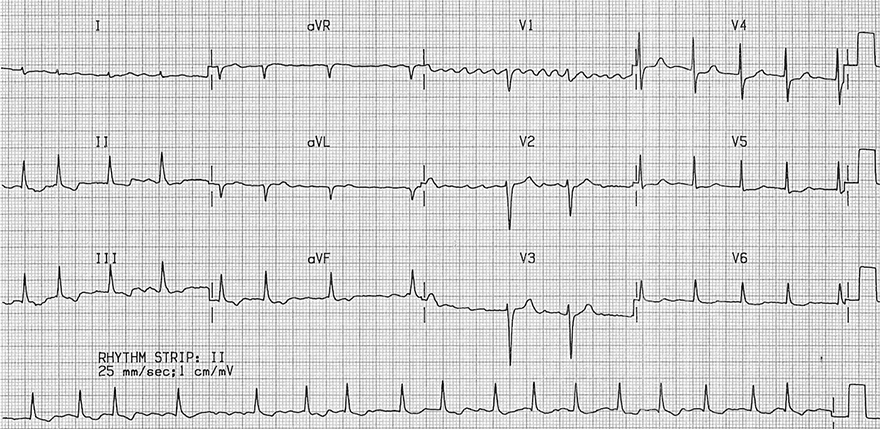
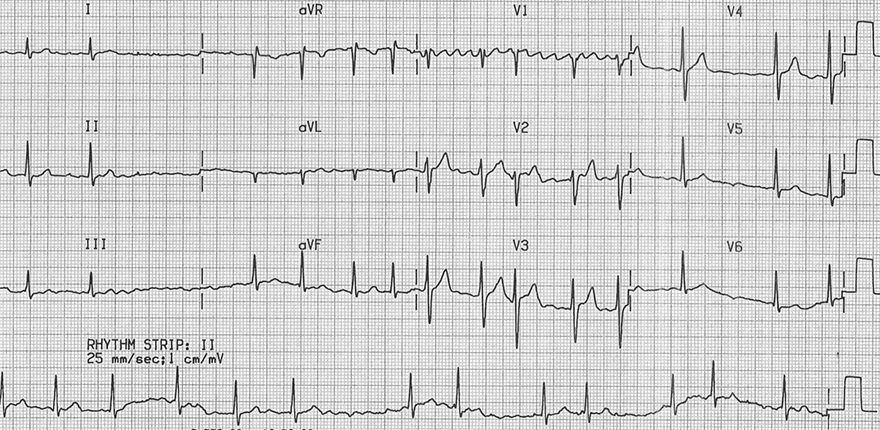
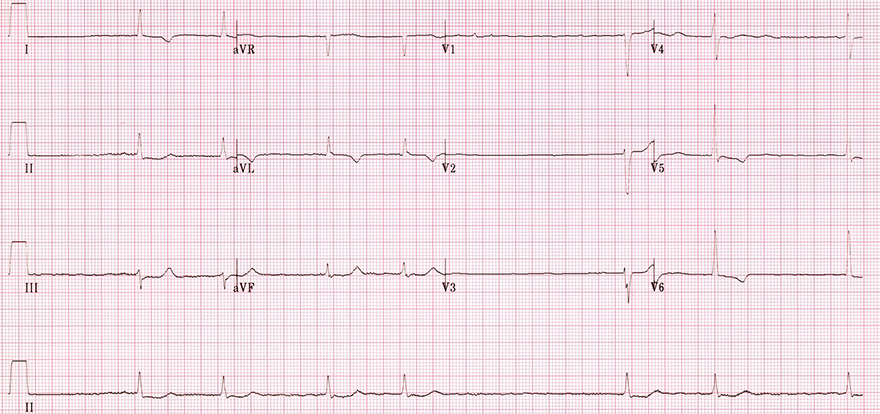
Atrial Fibrillation
Atrial Fibrillation and Frequency 130/min.
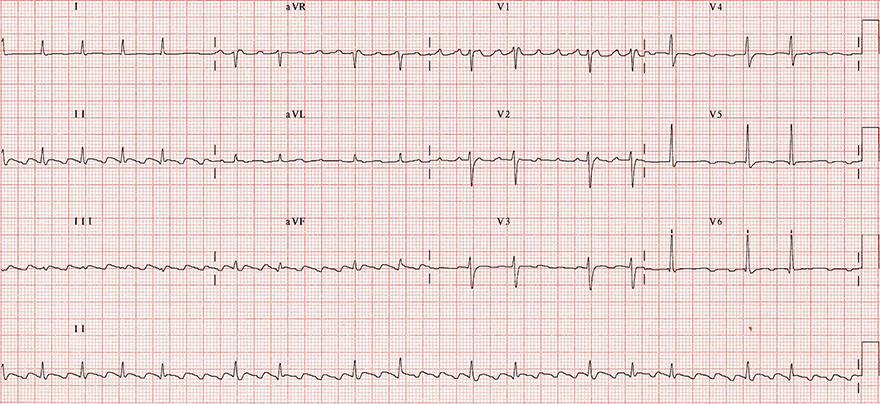
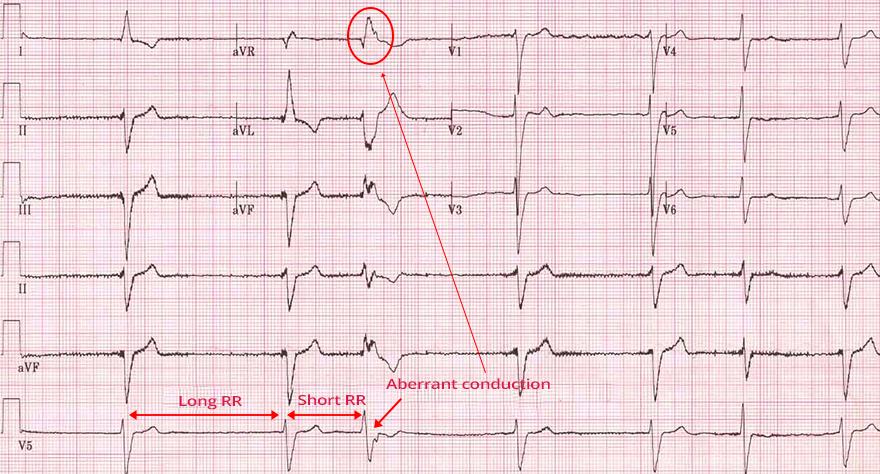
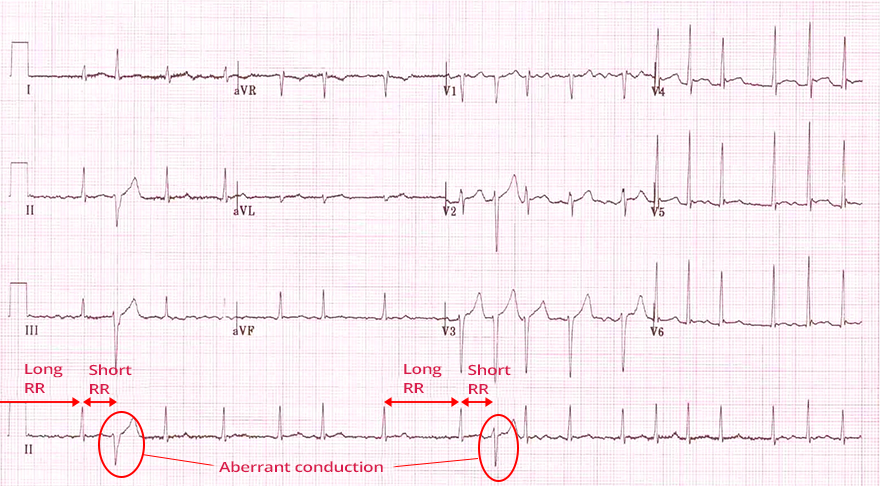
Ashman Phenomenon and Atrial Fibrillation
|
|
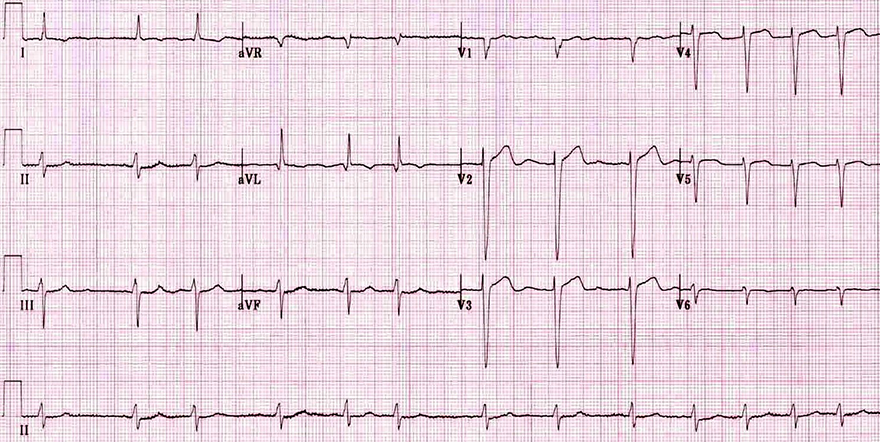
Atrial Fibrillation
|
|
|
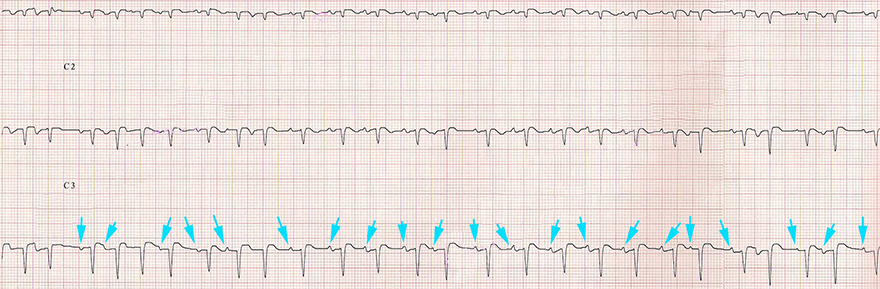
Atrial Flutter with Variable Conduction (2:1 and 4:1)
|
|
|
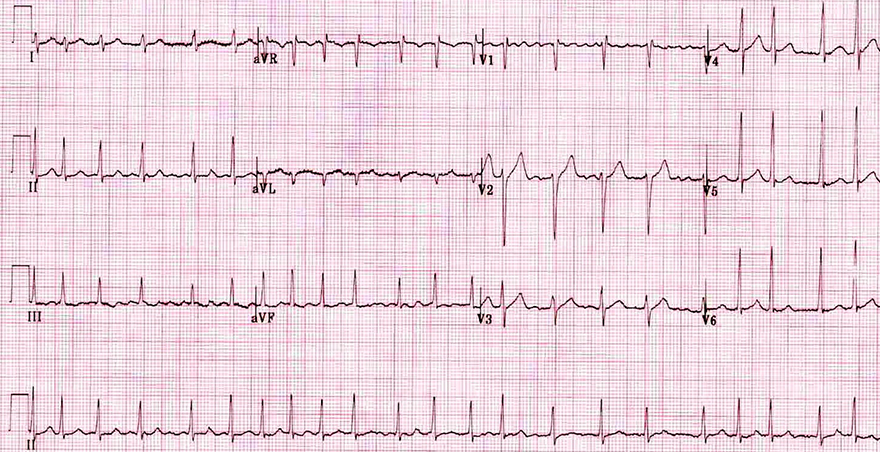
Multifocal Atrial Tachycardia
|
Atrial Fibrillation
Atrial Flutter (with Variable Conduction 2:1 and 4:1)
Atrial Fibrillation
Atrial Fibrillation
Multifocal Atrial Tachycardia
Atrial Fibrillation
Atrial Fibrillation
Atrial Fibrillation and Ashman’s Phenomenon
Atrial Fibrillation and Ashman’s Phenomenon
Sources