Home /
Atrial Flutter
Atrial Flutter (AFL)
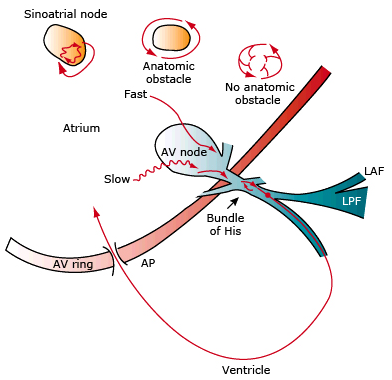
Re-entry and Supraventricular Tachycardia
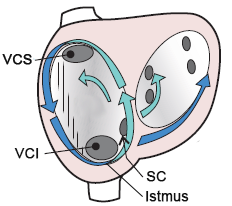
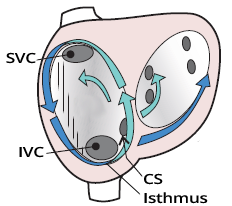
Anatomy of the Right Atrium
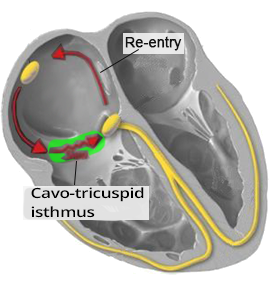
- Cavotricuspid Isthmus
- Isthmus (from Greek "narrow strip of land in the sea")
- The isthmus is a narrow band of fibrous tissue that separates:
- the mouth of the inferior vena cava (IVC) and
- the tricuspid annulus
- In atrial flutter, it forms a slow pathway for re-entry
- Tricuspid Annulus
- It is a fibrous ring
- It forms the supporting skeleton for the tricuspid valve
- Crista Terminalis (CT)
- It is a narrow strip of muscle
- between the openings of the superior and inferior vena cava
- It separates the appendage of the right atrium
- Superior Vena Cava (SVC) is the upper vena cava
- Inferior Vena Cava (IVC) is the lower vena cava
- Coronary Sinus (CS)
- It is the main venous drainage trunk of the heart
- It opens into the right atrium
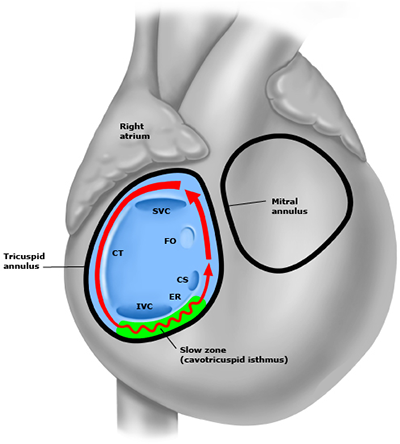
- Foramen Ovale (FO)
- It is an opening in the atrial septum
- During embryonic development, it connects the atria, later it closes
- In 20% of people, it does not completely close but usually does not cause problems
- Eustachian Ridge (ER)
- The Eustachian ridge directs blood from the inferior vena cava to the foramen ovale during embryonic development
- It facilitates the direct passage of oxygenated blood into the circulation
- The Eustachian ridge later disappears and only the Eustachian ridge remains
Atrial Flutter
- It almost always occurs in a structurally altered right atrium
- In the right atrium, there is a macro re-entry circuit
- Through which the impulse circulates at a frequency of approximately 300/min (200 - 400/min)
- The impulse passes through the AV node to the ventricles most commonly in a ratio of 2:1
- The impulse circulates twice in the macro re-entry (in the right atrium)
- and passes once to the ventricles
- The atria beat at 300/min, and the ventricles at 150/min
- This is a protective mechanism of the AV node (through the refractory period)
- Atrial flutter with 1:1 conduction can occur in WPW syndrome
- If the patient receives medications to slow the AV node
- Impulses from the atrium then reach the ventricles through an accessory pathway
- Which does not have the protective mechanism of the AV node
- The ventricles are activated at 300/min and ventricular fibrillation occurs
- Atrial flutter and atrial fibrillation
- Can cause embolic stroke
- At high atrial frequencies, blood stagnates in the atria
- and thrombi (blood clots) form
- Atrial flutter (300/min - atrial frequency)
- Atrial fibrillation (350-600/min - atrial frequency)
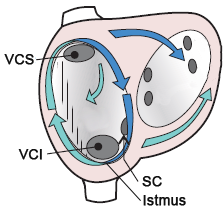
Typical Flutter (Isthmus-Dependent)
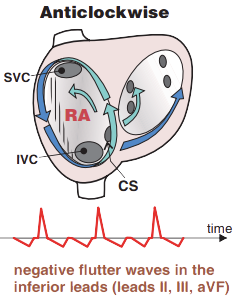
Typical atrial flutter, Anticlockwise atrial flutter
- Sometimes referred to as Type I atrial flutter
- This is the most common form of atrial flutter (90% of cases)
- Macro re-entry occurs through the cavotricuspid isthmus
- The impulse circulates through the re-entry circuit at a frequency of 240-340/min
- The impulse circulates counterclockwise (Anticlockwise re-entry)
- Characteristic sawtooth waves (F-waves) are seen on the ECG, instead of P waves
Reverse Typical Flutter (Isthmus-Dependent)
Reverse Typical Atrial Flutter, Clockwise Atrial Flutter
- Sometimes referred to as Reverse Type I atrial flutter
- It is very rare (< 10% of cases)
- Macro re-entry occurs through the cavotricuspid isthmus
- The impulse circulates through the re-entry circuit at a frequency of 240-340/min
- The impulse circulates clockwise (Clockwise re-entry)
- Characteristic sawtooth waves (F-waves) are seen on the ECG, instead of P waves
ECG and Atrial Flutter

- Narrow QRS complexes (because impulses are conducted to the ventricles through the AV node)
- Atrial frequency is approximately 300/min
- Isthmus-dependent flutter: 240-340/min (90% of cases)
- Isthmus-independent flutter: 340-440/min (< 10% of cases)
- In the inferior leads (II, III, aVF) there are "sawtooth waves"
- An isoelectric line is not present
- Flutter (F) waves (sawtooth waves) may resemble P waves in V1
How Flutter (F) Waves (Sawtooth Waves) Are Formed

- The impulse circles through macro re-entry with a frequency of approximately 300/min
- Therefore, flutter waves have a frequency of 300/min
- Sawtooth waves (F waves) are produced only by Isthmus-Dependent Flutter
- Because macro re-entry covers almost the entire right atrium
- The impulse circles around the AV node
- Thus, the impulse is almost directly TOWARDS or AWAY FROM
- inferior leads (II, III, aVF)
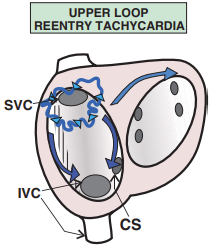
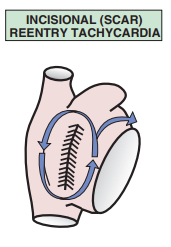
- Atypical Flutter
- Has macro re-entry but does not pass through the isthmus (around the AV node)
- The re-entry vector does not create sawtooth waves
ECG and Typical Flutter (Isthmus-Dependent)
- This is the most common atrial flutter (90% of cases)
- The impulse circles through re-entry across the isthmus around the AV node with a frequency of approximately 300/min
- The impulse circles through re-entry in a direction AWAY FROM the inferior leads
- In the inferior leads (II, III, aVF)
- negative flutter waves (sawtooth waves) appear
- Positive waves appear in V1
- Because the V1 lead is "opposite" the inferior leads
Reverse Typical Flutter (Isthmus Dependent)
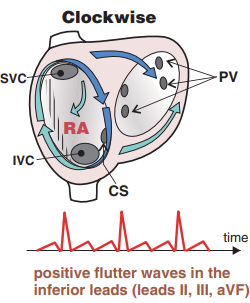
- It is very rare (< 10% of cases)
- The impulse circulates through re-entry across the isthmus around the AV node with a frequency of approximately 300/min.
- The impulse circulates through re-entry in the upward direction in the inferior leads
- Therefore, in inferior leads (II, III, aVF)
- positive Flutter waves (sawtooth) are observed
- In V1, negative waves are observed
- Because lead V1 is "opposite" to the inferior leads
Conduction to the Ventricles
- Isthmus-dependent flutter has a re-entry frequency of approximately 300/min.
- The AV node blocks the conduction of impulses to the ventricles
- This is a functional block - a protective mechanism of the AV node, protecting the ventricles from extreme tachycardia
- This is not an organic AV block (due to damage to the AV node)
- The functional AV block or conduction to the ventricles can have varying degrees
- Ventricular frequency (QRS) with atrial flutter at a frequency of 300/min. will depend on the conduction ratio:
- Conduction 2:1 = ventricles at 150/min.
- Conduction 3:1 = ventricles at 100/min.
- Conduction 4:1 = ventricles at 75/min.
- Atrial flutter can also have variable AV block (conduction to the ventricles)
- On the ECG, this results in a varying conduction ratio of 2:1, 3:1, 4:1
- Flutter then resembles atrial fibrillation because the heart action (QRS) is irregular
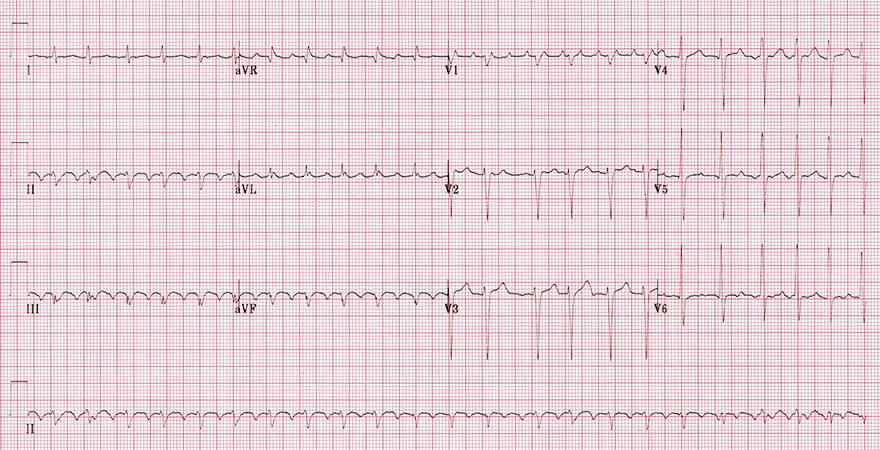
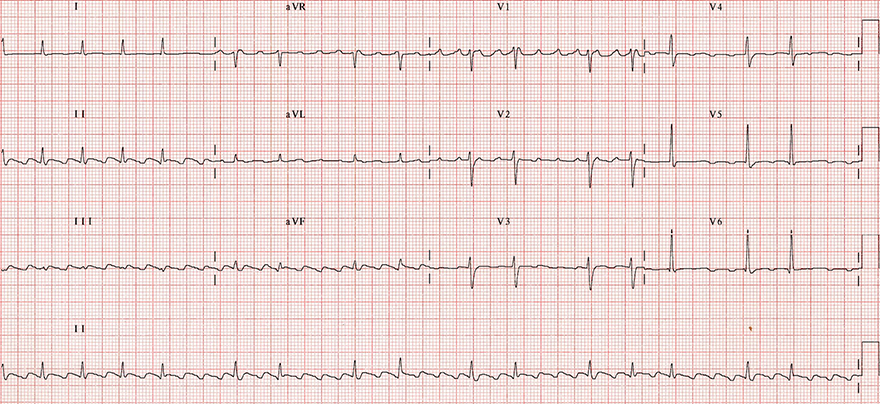
Atrial Flutter (3:1)
- Frequency: 140/min.
- Atrial frequency: 280/min.
- Ventricular frequency: 140/min.
- Notice the characteristic sawtooth waves
- This is istmus-dependent flutter (frequency is 240-340/min.)

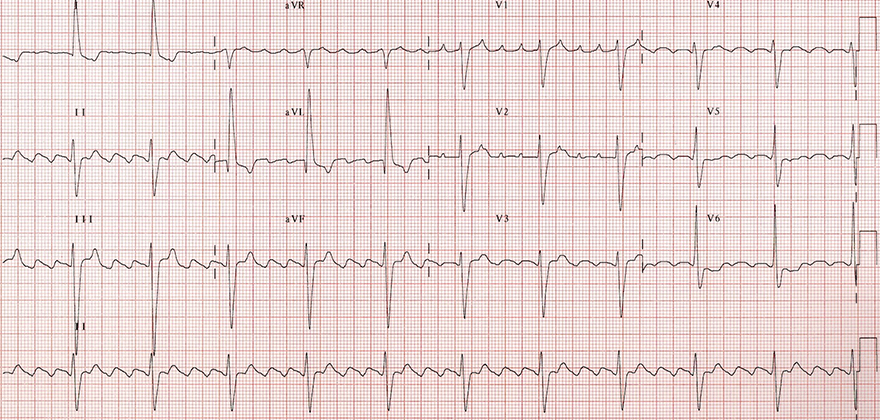
Atrial Flutter (4:1)
- Frequency: 68/min.
- Atrial frequency: 272/min.
- Ventricular frequency: 68/min.
- Note that this is not a 3:1 block; the block to the ventricles is 4:1
- Notice the peaks of the flutter waves, which are oriented downward
- This is again istmus-dependent flutter (frequency is 240-340/min.)

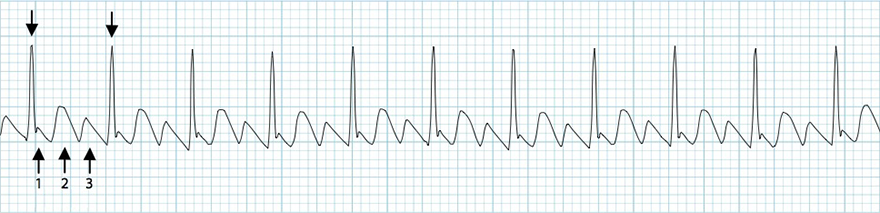
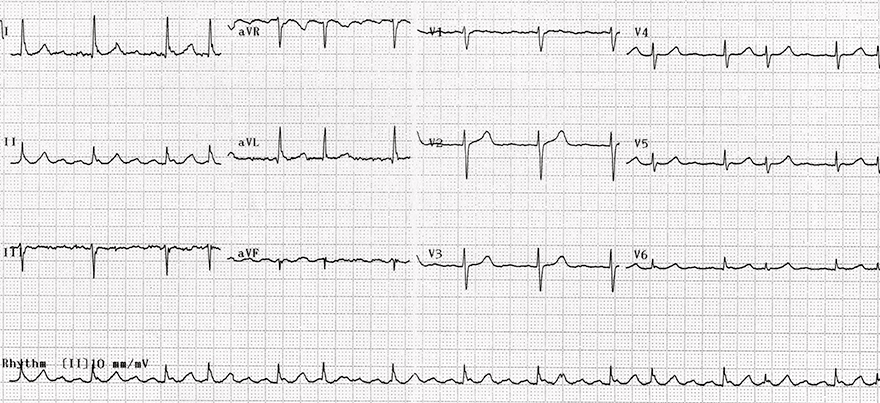
Atrial Flutter (with variable AV block of 2:1 and 4:1)
- Frequency (QRS): 90/min. (6-second method)
- Flutter wave frequency: 300/min.
- This is istmus-dependent flutter (frequency is 240-340/min.)
- Ventricular frequency is regularly irregular. This means that 2 RR intervals alternate
- RR interval with 2:1 block
- RR interval with 4:1 block

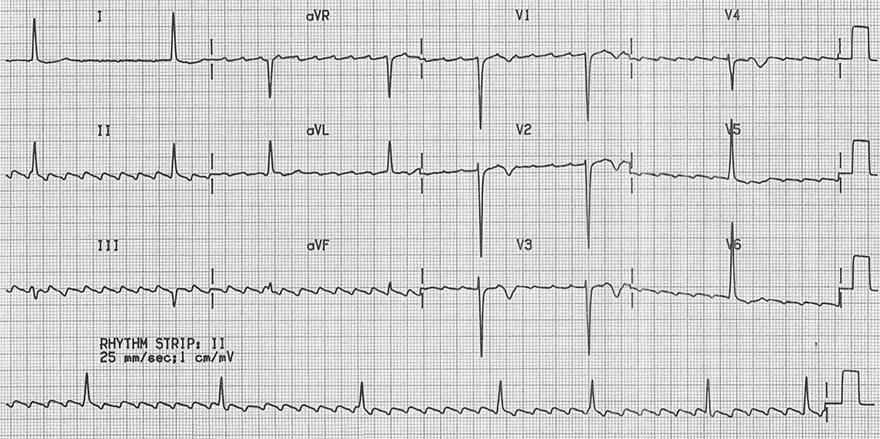
Atrial Flutter (with variable AV block of 7:1, 8:1, and 5:1)
- Frequency (QRS): 40/min. (6-second method)
- Flutter wave frequency: 300/min.
- This is istmus-dependent flutter with variable AV block (7:1, 8:1, 5:1)
Laddergram and Atrial Flutter
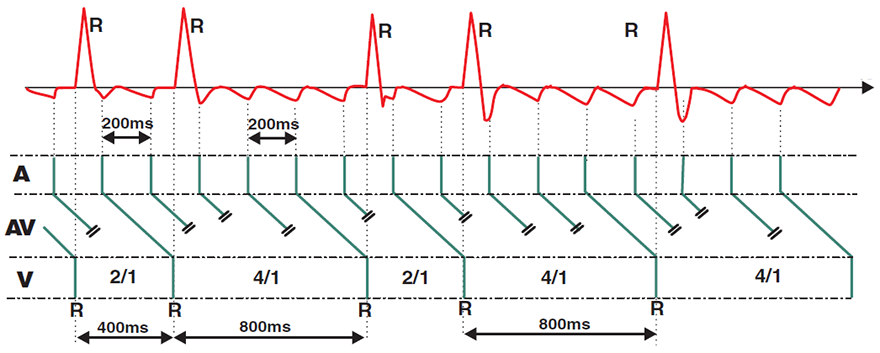
Typical Atrial Flutter (Isthmus-dependent) with variable block 2:1 and 4:1
- Laddergram illustrates the propagation of impulses through the conducting system
- A - atria, AV - AV node, V - ventricles
- On the ECG, this is Typical Atrial Flutter (impulse circulates counterclockwise through the isthmus)
- Atrial frequency is 300/min.
- One circuit (1 F wave) lasts 200ms (0.2s)
- 5 F waves occur in 1 second
- 300 F waves occur in 1 minute
- Impulses arrive at the AV node with a frequency of 300/min.
- The AV node allows impulses to pass to the ventricles with variable block of 2:1 and 4:1
- RR interval (ventricles) always forms X times F waves
- 2x200ms = 400ms
- 4x200ms = 800ms
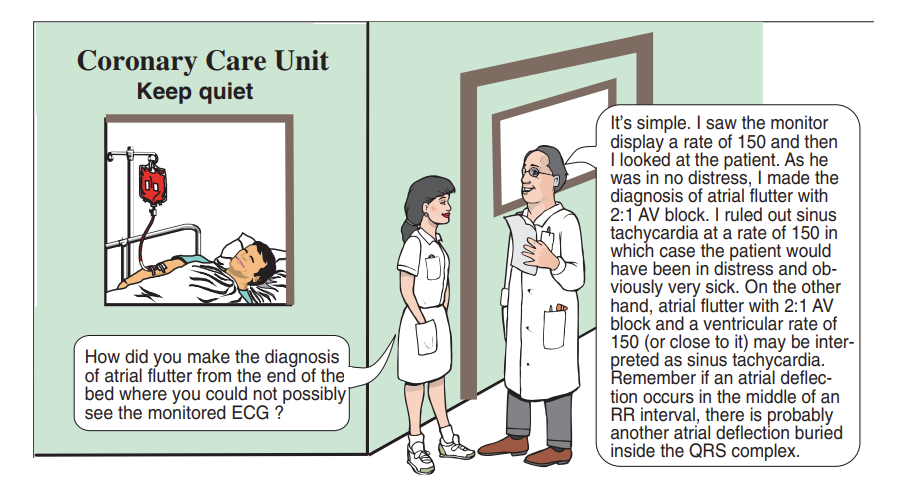
Rapid Diagnosis - Atrial Flutter
- Atrial Flutter is likely if:
- There is supraventricular tachycardia with a frequency of 130-170/min.
- Sawtooth waves (Flutter waves) are present in the inferior leads (II, III, aVF)
- QRS complexes are regularly irregular
- The patient has minimal subjective symptoms (not feeling faint, no fever, breathing well, etc.)
- Increase in AV node block
- RR Interval
- Atrial flutter with variable AV block can resemble atrial fibrillation
- Because the RR interval changes irregularly but is regularly irregular
- Because the RR interval in flutter is always X times the FF interval
Atrial Flutter (2:1)
- Typical Isthmus-dependent flutter
- The impulse circles counterclockwise through the isthmus
- Inverted flutter waves in the inferior leads (II, III, aVF) with a frequency of 300/min.
- Positive flutter waves in V1 (resembling a P wave)
- Conduction to the ventricles is 2:1 (or AV block is 2:1)
- Ventricular frequency 150/min.
- Irregularity of QRS (V1-V3)
- Caused by intermittently variable conduction to the ventricles 3:1
- This is a flutter with 2:1 conduction
- because a 3:1 conduction is very rare in this ECG

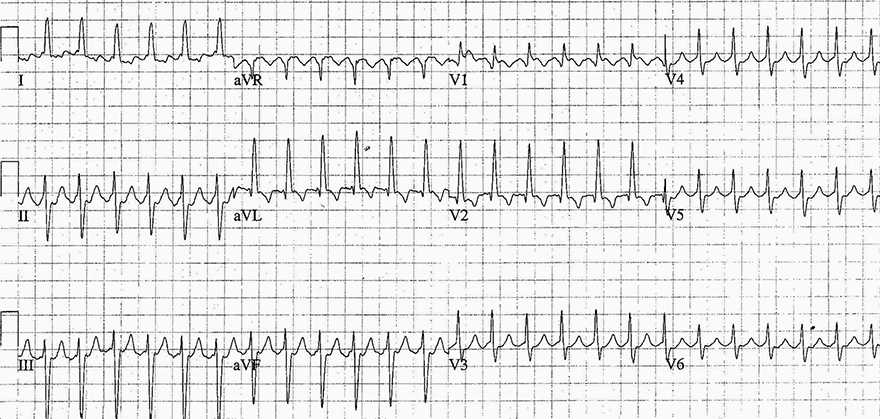
Atrial Flutter (2:1)
- Supraventricular Tachycardia (SVT) with a frequency of 150/min.
- Any SVT with a frequency of 150/min. has a high suspicion of being Atrial Flutter (2:1)
- In V1, negative flutter waves with a frequency of 300/min.
- The patient experienced only discrete palpitations (heart pounding)
- This is a reverse typical atrial flutter
- The impulse circles in a clockwise direction through the isthmus
- Atrial flutter with 2:1 conduction
- Often has flutter waves embedded in T waves
- If the flutter F waves cannot be differentiated, we must rule out other SVTs
Atrial Flutter (2:1)
- Flutter waves can sometimes be difficult to differentiate in flutter with 2:1 conduction
- Atrial Flutter (2:1)
- Has extremely regular QRS complexes with a frequency of about 150/min.
- AVNRT and AVRT have frequencies of 170-250/min.
- Vagal maneuvers, or adenosine (slow conduction through the AV node)
- AVNRT / AVRT often revert to sinus rhythm
- Atrial Flutter (2:1) increases AV block, for example, to 3:1 and unveils flutter waves
- Sinus tachycardia slows down and P waves become visible

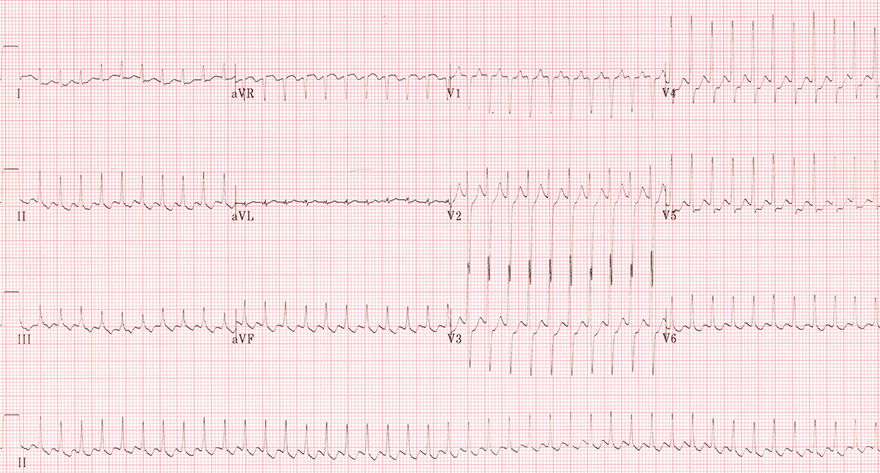
Atrial Flutter (After Administration of Adenosine)
- The patient had supraventricular tachycardia with a frequency of 150/min.
- This EKG does not show it
- After administering Adenosine, the following EKG was recorded - flutter waves were unmasked
- The patient had on the preceding EKG (which we do not see)
- Atrial flutter with 2:1 conduction and a frequency of 150/min.
- AV block also increases with vagal maneuvers
- However, vagal maneuvers do not induce as high an AV block as Adenosine
- During carotid sinus massage, atrial flutter would be unmasked
- with a lower conduction ratio (e.g., 3:1)

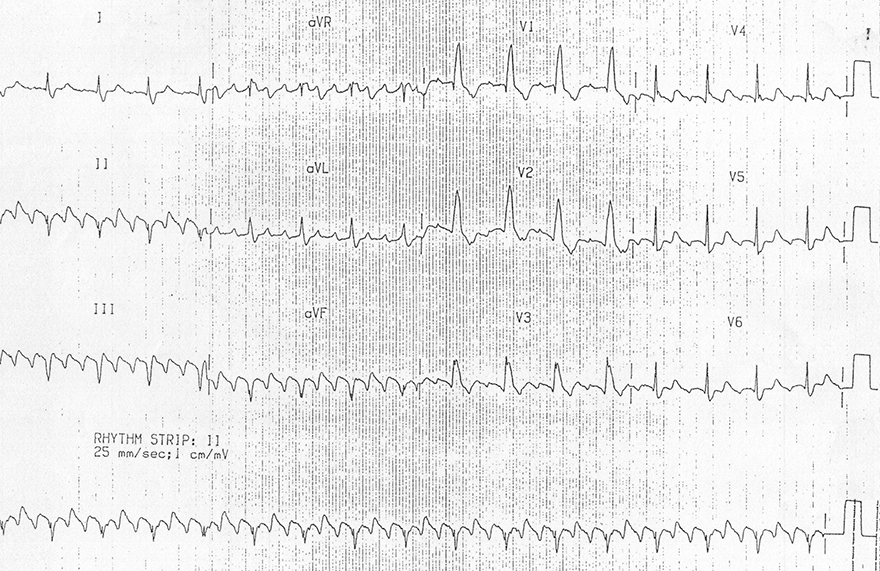
AVNRT and Conversion to Sinus Rhythm After Adenosine
- Initially, there is supraventricular tachycardia with a frequency of 150/min.
- There is a high suspicion that it is atrial flutter with 2:1 conduction
- However, flutter waves could not be differentiated even on a 12-lead EKG
- After administering Adenosine
Atrial Flutter (with Variable Conduction 2:1 and 4:1)
- Typical Isthmus-Dependent Flutter
- The impulse circulates counterclockwise through the isthmus
- Inverted flutter waves in the inferior leads (II, III, aVF) with a frequency of 300/min
- Positive flutter waves in V1 (resembling P waves)
- Conduction to the ventricles alternates between 2:1 and 4:1 (note the continuous lead II)
- RR interval with 4:1 block is exactly twice the RR interval with 2:1 block
- Ventricular frequency is regularly irregular (alternating between 2 RR intervals):
- 1. RR interval with 2:1 conduction
- 2. RR interval with 4:1 conduction
Atrial Flutter (4:1)
- Typical Isthmus-Dependent Flutter
- The impulse circulates counterclockwise through the isthmus
- Inverted flutter waves in the inferior leads (II, III, aVF) with a frequency of 260/min
- Positive flutter waves in V1 and V2 (resembling P waves)
- Conduction to the ventricles is 4:1
Atrial Flutter (with Variable Conduction 2:1 and 4:1)
- Reversed Typical Isthmus-Dependent Flutter
- The impulse circulates clockwise through the isthmus
- Positive flutter waves in the inferior lead II with a frequency of 300/min
- Flutter waves cannot be differentiated in the V1 lead
- Conduction to the ventricles is 4:1
- Ventricular frequency: 75/min
- In the continuous inferior lead II, conduction 2:1 intermittently occurs
- Ventricular frequency with 2:1 conduction is approximately 150/min
Atrial Flutter (with High Degree AV Block)
- Typical Isthmus-Dependent Flutter
- The impulse circulates counterclockwise through the isthmus
- Inverted flutter waves in the inferior leads (II, III, aVF) with a frequency of 260/min
- Positive flutter waves in V1 and V2 (resembling P waves)
- Conduction to the ventricles alternates between 7:1, 8:1, and 5:1
Supraventricular Tachycardia
- On the EKG, supraventricular tachycardia with a rate of 250-300/min may be:
- Atrial Flutter with 1:1 conduction
- AVNRT
- AVRT
- Flutter waves are indicated in the inferior leads (II, III, aVF)
- A patient with a ventricular rate of 240-300/min is hemodynamically unstable
- Vagal maneuvers or adenosine will increase AV node block
- In atrial flutter, flutter waves would be demasked (since AV block would occur)
- In this case, urgent treatment with electrical cardioversion is indicated
Atrial Flutter (3:1)
- Typical Isthmus-dependent atrial flutter
- The impulse circulates counterclockwise through the isthmus
- Inverted flutter waves in the inferior leads (II, III, aVF) with a frequency of 300/min
- Positive flutter waves in V1
- Every 3rd flutter wave deforms the lower part of the T wave
- Ventricular conduction is 3:1
Sources
- ECG from Basics to Essentials Step by Step
- litfl.com
- ecgwaves.com
- metealpaslan.com
- medmastery.com
- uptodate.com
- ecgpedia.org
- wikipedia.org
- Strong Medicine
- Understanding Pacemakers