|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Home /
Atrioventricular reentrant tachycardia (AVRT), Atrioventricular reciprocating tachycardia, Orthodromic and Antidromic AVRT, Orthodromic Reciprocating Tachycardia (ORT)



Orthodromic AVRT

Antidromic AVRT

Orthodromic AVRT
Supraventricular Tachycardia (SVT)

WPW Syndrome

Orthodromic AVRT
PJRT

PJRT
Wide-Complex Tachycardia
WPW Syndrome

Orthodromic AVRT

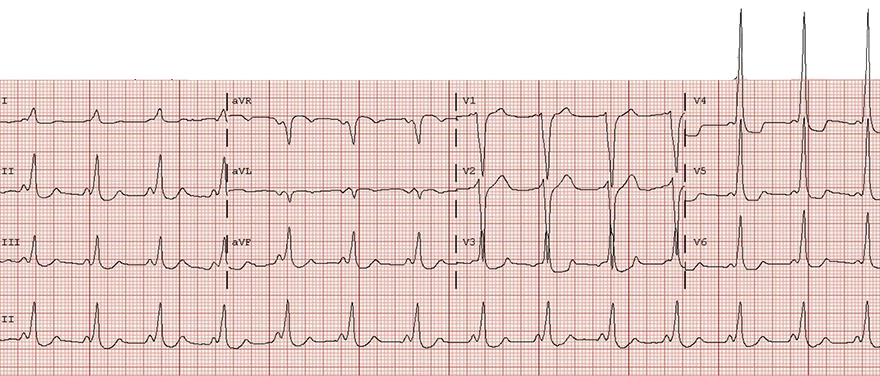
WPW Syndrome (Type A)

Orthodromic AVRT

WPW Syndrome (Type A)
Antidromic AVRT

WPW Syndrome (Type B)

Antidromic AVRT
WPW Syndrome (Type B)

Antidromic AVRT

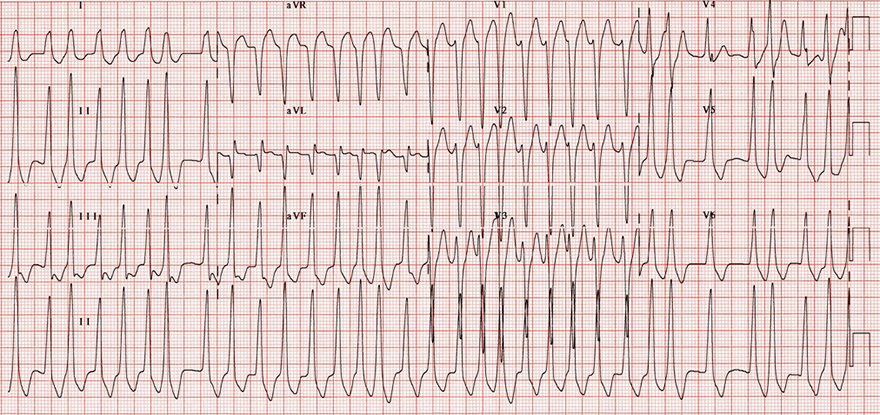
Antidromic AVRT and Atrial Fibrillation

Antidromic AVRT and Atrial Fibrillation
Sources
Home /
Atrioventricular reentrant tachycardia (AVRT), Atrioventricular reciprocating tachycardia, Orthodromic and Antidromic AVRT, Orthodromic Reciprocating Tachycardia (ORT)
|
|
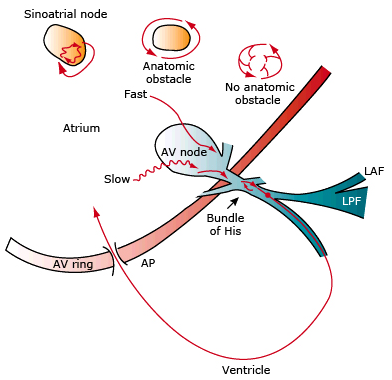
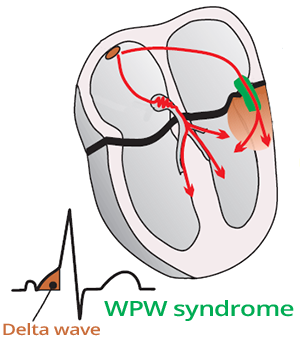
WPW Syndrome
|
|
|
|
|
|
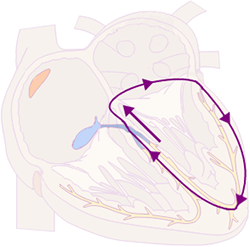
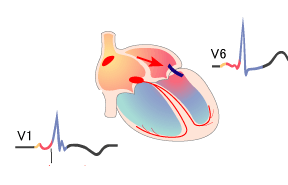
Orthodromic AVRT
|
|
|
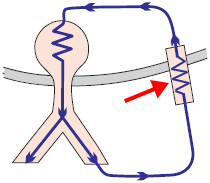
Antidromic AVRT
|
Orthodromic AVRT
Differential Diagnosis of AVRT
|
|
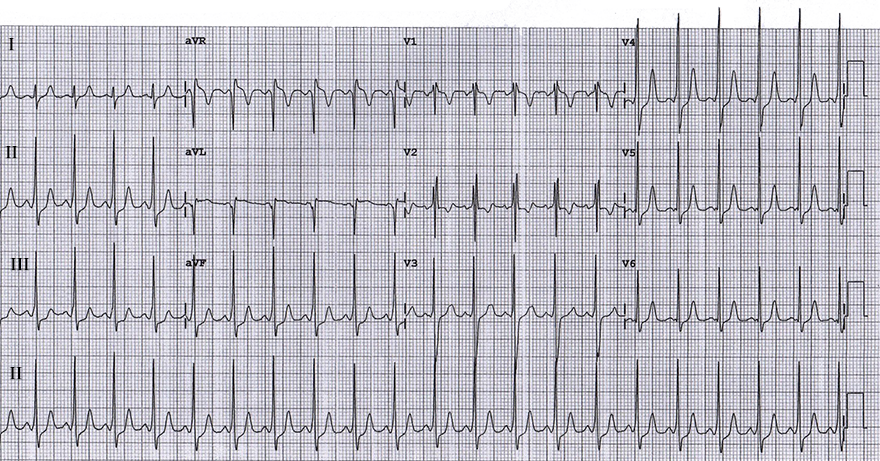
ECG and Orthodromic AVRT
|
|
Supraventricular Tachycardia (SVT)
WPW Syndrome
|
|
|
|
Orthodromic AVRT
|
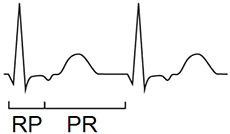
PJRT
|
PJRT
|
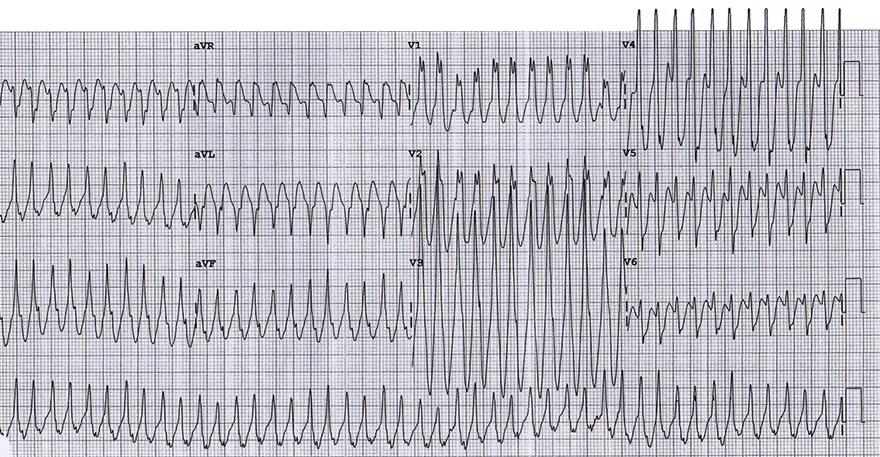
ECG and Antidromic AVRT
|
|
Wide-Complex Tachycardia
WPW Syndrome
Orthodromic AVRT
|
WPW Syndrome (Type A)
|
|
Orthodromic AVRT
|
WPW Syndrome (Type A)
|
|
Antidromic AVRT
|
WPW Syndrome (Type B)
|
|
Antidromic AVRT
|
WPW Syndrome (Type B)
|
|
Antidromic AVRT
|
Antidromic AVRT and Atrial Fibrillation
|
|
|
Antidromic AVRT and Atrial Fibrillation
|
|
Sources