|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
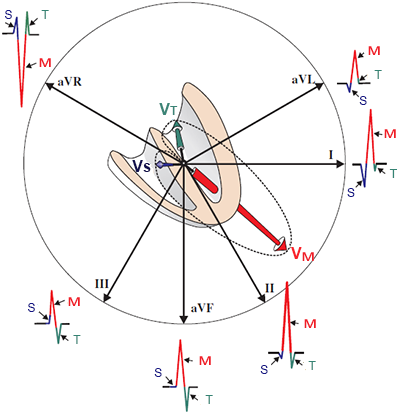
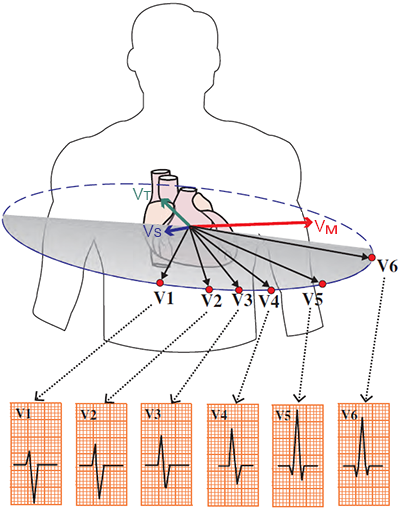
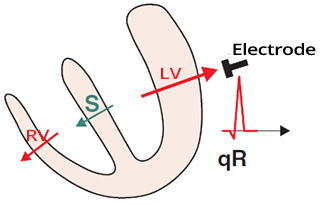
Physiological Q Wave

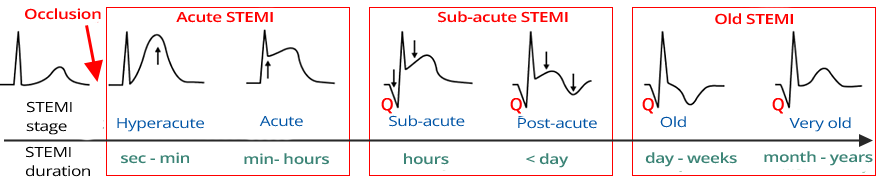
STEMI Stages
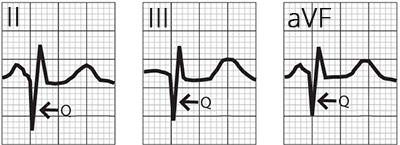
Old Inferior STEMI
| Etiology | Localization | |
| Myocardial Infarction (MI) (older term: Q infarction) |
Above the electrical window | After inferior MI, Q appears in (II, III, aVF); after anterior MI, Q appears in (V1-V3) |
| Left Bundle Branch Block (LBBB) | V1-V3, III, aVF | Impulse spreads to the right ventricle through the Tawara branch. Then, the impulse spreads to the left ventricle through the myocardium. The vector thus directs from the right ventricle to the left ventricle, from leads V1-V3, III, and aVF. |
| Left Anterior Hemiblock | II, III, aVF | The main cardiac vector turns away from leads II, III, aVF, where a pathological Q wave may occur |
| Left Posterior Hemiblock | I, aVL | The main cardiac vector turns away from leads I, aVL, where a pathological Q wave may occur |
| Pulmonary Embolism | III | Causes overload and dilation of the right heart. The main cardiac axis shifts to the right. 20% of patients with pulmonary embolism have a pathological Q wave in lead III. It causes the S1Q3T3 pattern |
| Infiltrative Diseases | V1-V3 | In amyloidosis, pathological proteins deposit in the myocardium, which may cause a pathological Q wave |
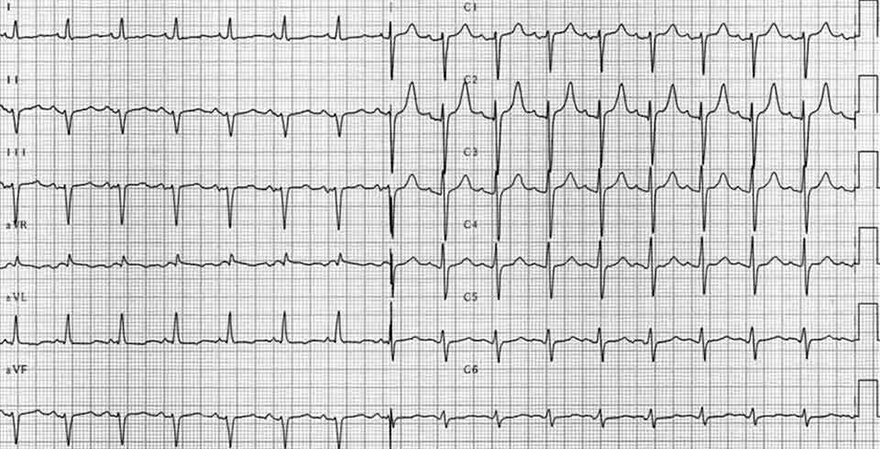
| WPW Syndrome | II, III, aVF | In WPW syndrome, ventricles are activated through two pathways (AV node and accessory pathway). Vectors in the ventricles can create a pathological Q wave |
| Myocarditis | Above a certain area of the heart | Myocarditis can cause pathological Q waves above a certain area of the heart |
| Cardiac Contusion | Above the affected area | Contusion (bruising) of the heart can cause a pathological Q wave |
| Chest Deformities | Above the affected area | Chest deformities may create a pathological Q wave due to altered electrical conduction |
| Misplaced Electrodes | I, aVL | Misplaced limb leads can produce a pathological Q wave |
| Hypertrophic Cardiomyopathy | (aVL, I, V5, V6), or (II, III, aVF) |
Hypertrophy of the ventricular septum can increase the septal vector and cause a pathological Q wave |
| Positional Q Waves | III | Positional Q waves appear in lead III during deep expiration, due to the rotation of the heart as the main cardiac vector turns away from lead III |
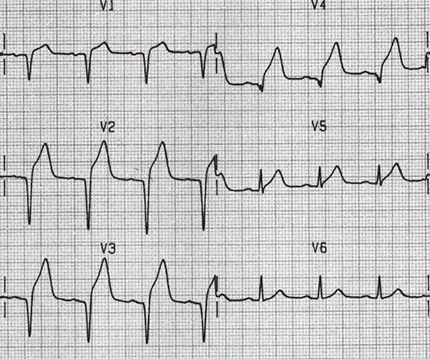
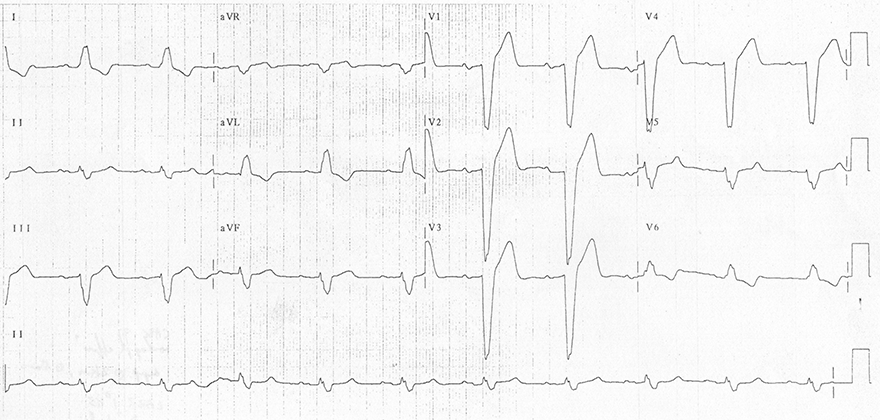
Subacute Antero-Septal Infarction
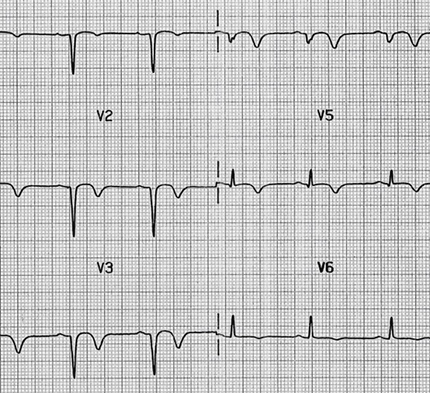
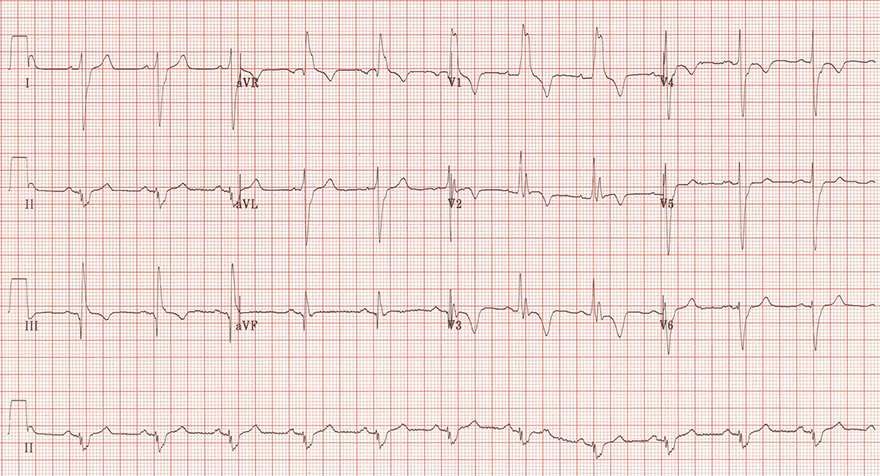
Old Antero-Septal Infarction
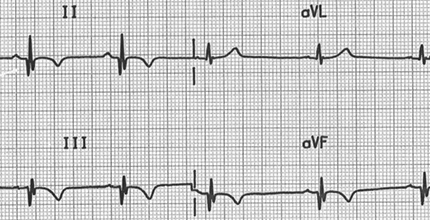
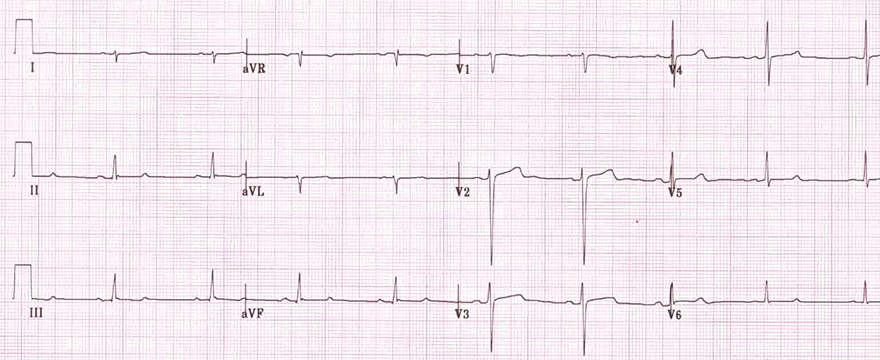
Old Inferior Infarction
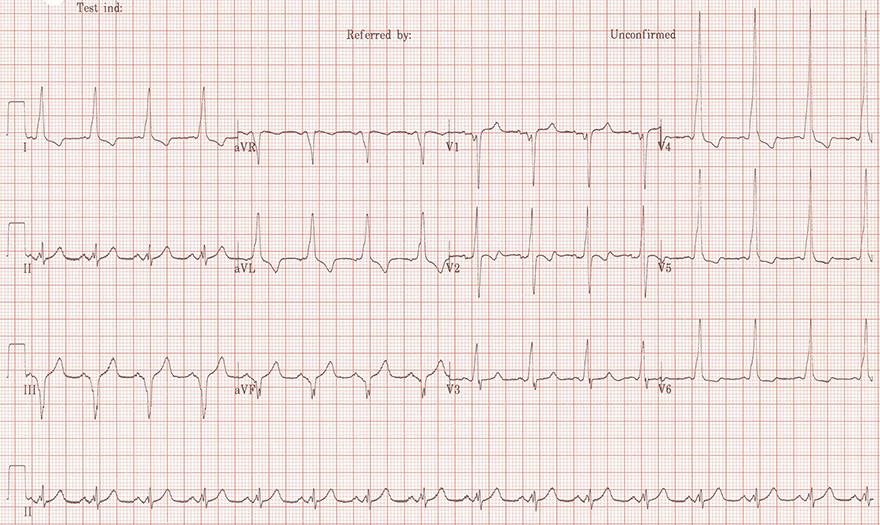
Left Bundle Branch Block
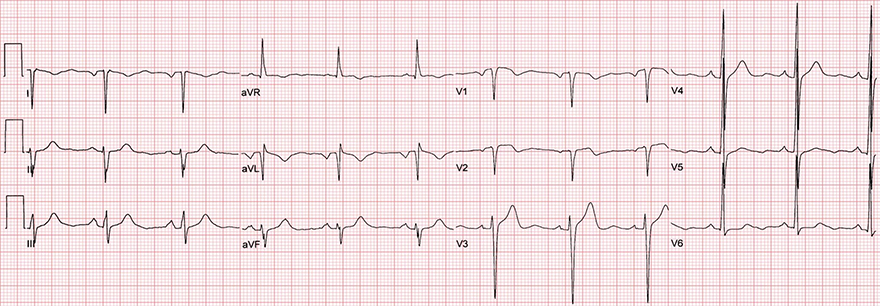
Left Anterior Fascicular Block
Left Posterior Fascicular Block
Acute Pulmonary Embolism
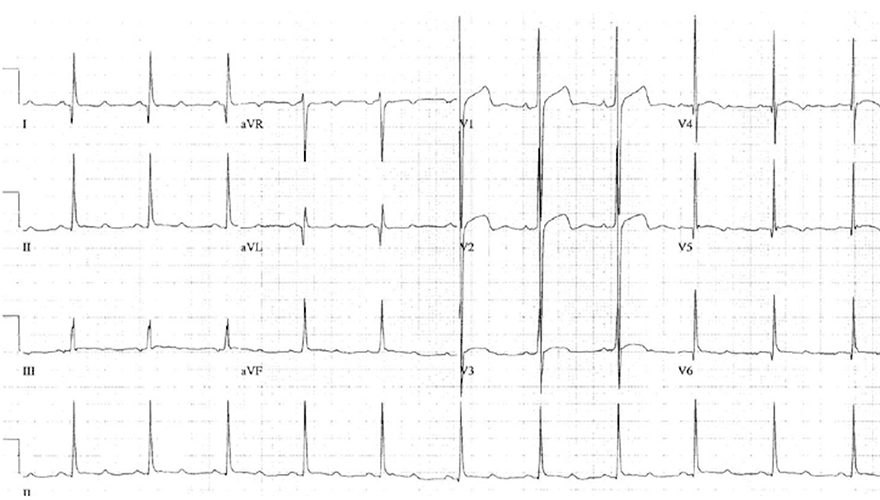
WPW Syndrome
Swapped ECG Leads on the Arms
Hypertrophic Cardiomyopathy
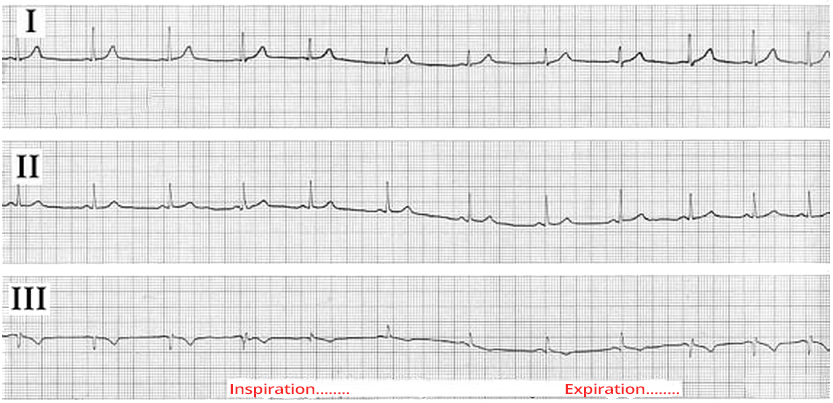
Positional (Respiratory) Q
Sources
Physiological Q Wave
|
|
Physiological Q Wave
ECG and Physiological Q Wave
|
|
|
|
STEMI Stages
|
Old Inferior STEMI
|
| Etiology | Localization | |
| Myocardial Infarction (MI) (older term: Q infarction) |
Above the electrical window | After inferior MI, Q appears in (II, III, aVF); after anterior MI, Q appears in (V1-V3) |
| Left Bundle Branch Block (LBBB) | V1-V3, III, aVF | Impulse spreads to the right ventricle through the Tawara branch. Then, the impulse spreads to the left ventricle through the myocardium. The vector thus directs from the right ventricle to the left ventricle, from leads V1-V3, III, and aVF. |
| Left Anterior Hemiblock | II, III, aVF | The main cardiac vector turns away from leads II, III, aVF, where a pathological Q wave may occur |
| Left Posterior Hemiblock | I, aVL | The main cardiac vector turns away from leads I, aVL, where a pathological Q wave may occur |
| Pulmonary Embolism | III | Causes overload and dilation of the right heart. The main cardiac axis shifts to the right. 20% of patients with pulmonary embolism have a pathological Q wave in lead III. It causes the S1Q3T3 pattern |
| Infiltrative Diseases | V1-V3 | In amyloidosis, pathological proteins deposit in the myocardium, which may cause a pathological Q wave |
| WPW Syndrome | II, III, aVF | In WPW syndrome, ventricles are activated through two pathways (AV node and accessory pathway). Vectors in the ventricles can create a pathological Q wave |
| Myocarditis | Above a certain area of the heart | Myocarditis can cause pathological Q waves above a certain area of the heart |
| Cardiac Contusion | Above the affected area | Contusion (bruising) of the heart can cause a pathological Q wave |
| Chest Deformities | Above the affected area | Chest deformities may create a pathological Q wave due to altered electrical conduction |
| Misplaced Electrodes | I, aVL | Misplaced limb leads can produce a pathological Q wave |
| Hypertrophic Cardiomyopathy | (aVL, I, V5, V6), or (II, III, aVF) |
Hypertrophy of the ventricular septum can increase the septal vector and cause a pathological Q wave |
| Positional Q Waves | III | Positional Q waves appear in lead III during deep expiration, due to the rotation of the heart as the main cardiac vector turns away from lead III |
|
|
|
|
Subacute Antero-Septal Infarction
|
Old Antero-Septal Infarction
|
Old Inferior Infarction
Left Bundle Branch Block
Left Anterior Fascicular Block
Left Posterior Fascicular Block
Acute Pulmonary Embolism
WPW Syndrome
Swapped ECG Leads on the Arms
Hypertrophic Cardiomyopathy
Positional (Respiratory) Q
Sources