|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
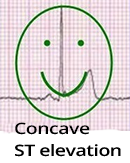

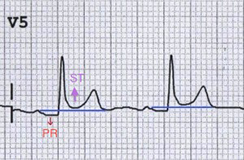
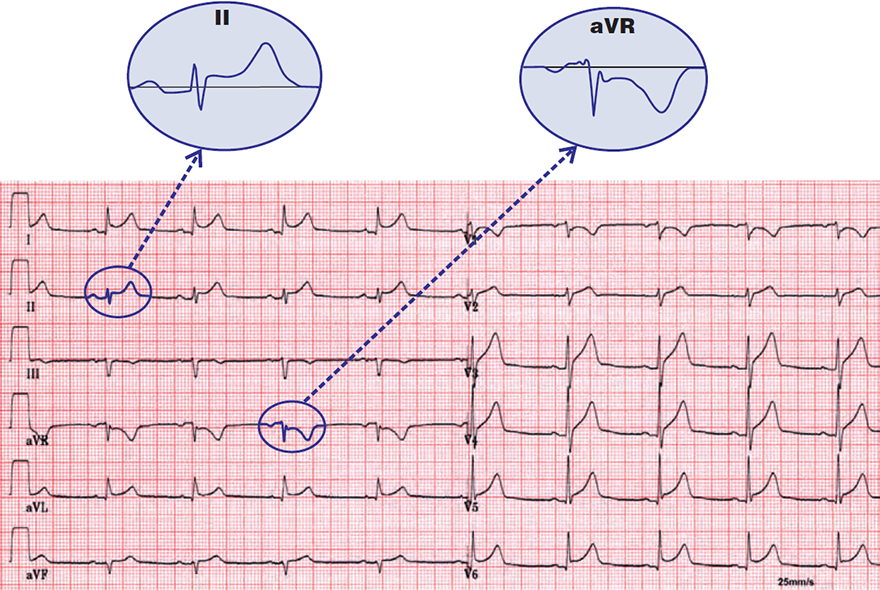
ST Elevations and PQ Depressions

ST Depressions and PQ Elevations

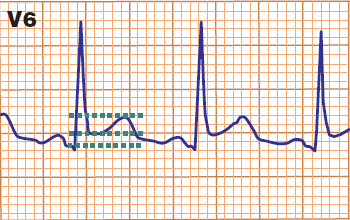
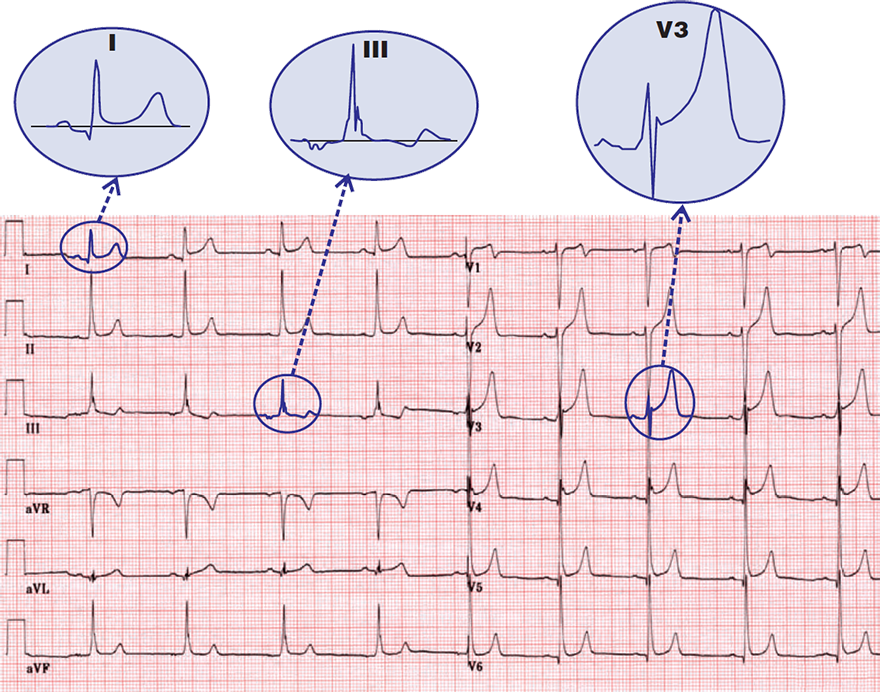
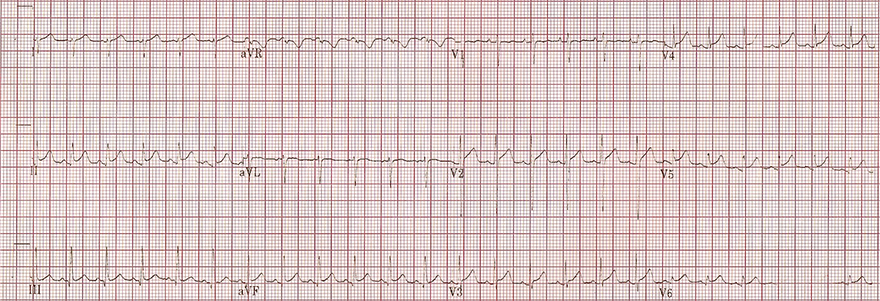
Spodick's Sign
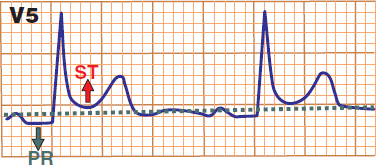
ST Elevations and PQ Depressions
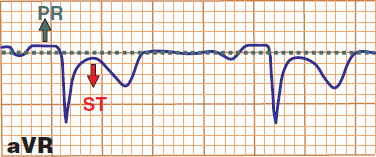
ST Depressions and PQ Elevations

Pericarditis and QRS Alternans


Pericarditis
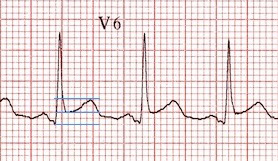
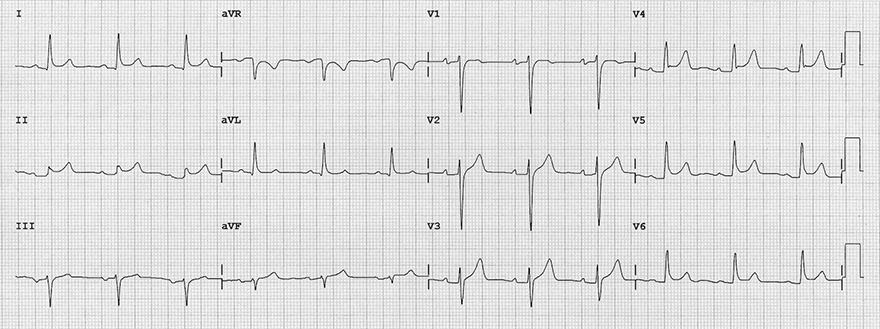
Benign Early Repolarization

Fishhook Pattern
Pericarditis

Benign Early Repolarization
Pericarditis

Benign Early Repolarization
Acute Pericarditis
Benign Early Repolarization
Acute Pericarditis

Acute Pericarditis

Acute Pericarditis
Acute Myopericarditis

Acute Myopericarditis
Benign Early Repolarization
Benign Early Repolarization + Pericarditis

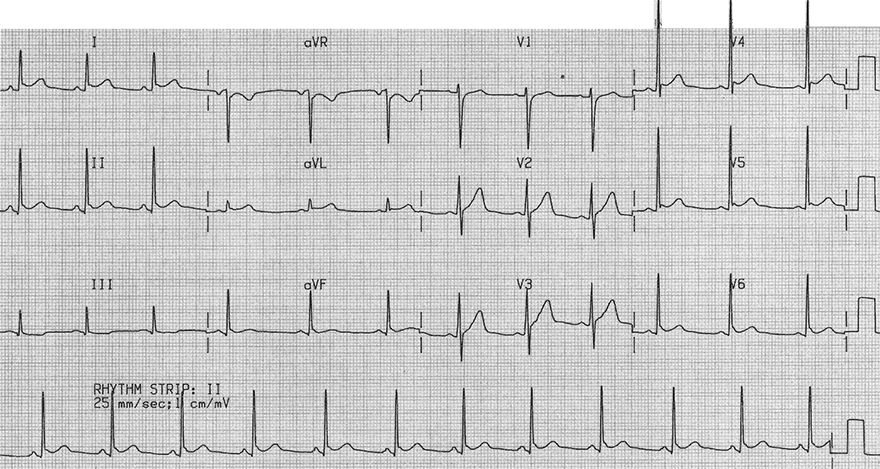
Acute Inferior STEMI Myocardial Infarction

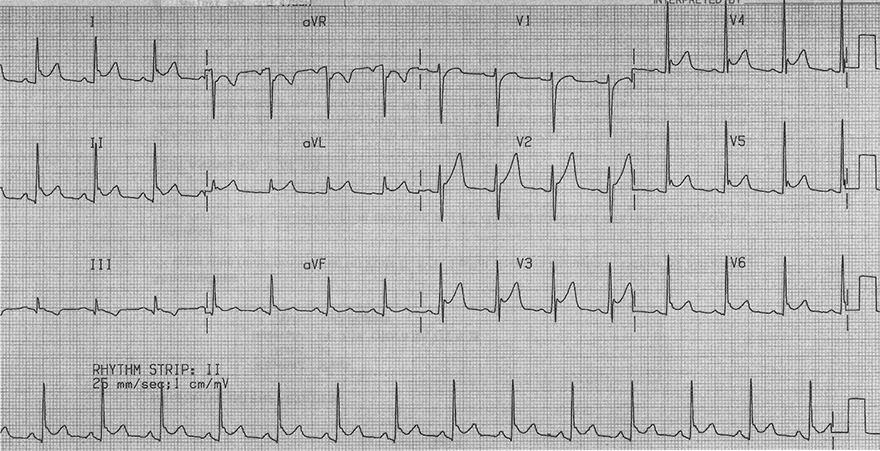
Acute Antero-Lateral STEMI
Sources
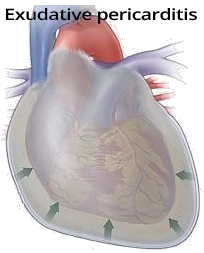
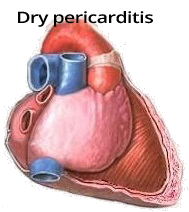
Pericardium and Pericarditis
|
|
ECG and Acute Pericarditis
|
|
|
ST Elevations and PQ Depressions
|
ST Depressions and PQ Elevations
|
Spodick's Sign
|
|
ST Elevations and PQ Depressions
|
ST Depressions and PQ Elevations
|
Pericarditis and QRS Alternans
|
|
Stage 1 (First 2 Weeks)
|
|
|
Stage 2 (Week 1-3)
|
|
|
Stage 3 (From Week 3 Onward)
|
|
|
Stage 4 (From Week 4 Onward)
|
Pericarditis vs. STEMI Infarction
|
|
Pericarditis vs. Benign Early Repolarization
|
|
|
Pericarditis
|
Benign Early Repolarization
|
|
|
Fishhook Pattern
|
|
|
|
Pericarditis
|
Benign Early Repolarization
|
|
|
|
Pericarditis
|
Benign Early Repolarization
|
Acute Pericarditis
Benign Early Repolarization
Acute Pericarditis
Acute Pericarditis
Acute Pericarditis
Acute Myopericarditis
Acute Myopericarditis
Benign Early Repolarization
Benign Early Repolarization + Pericarditis
Acute Inferior STEMI Myocardial Infarction
Acute Antero-Lateral STEMI
Sources