|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
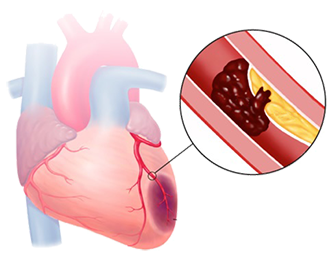
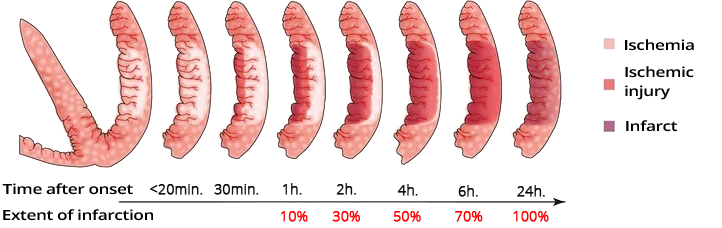
Dynamics of Ischemia After Occlusion
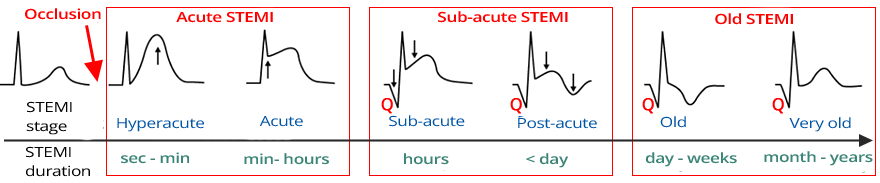
ECG Dynamics of STEMI Infarction

Old Inferior STEMI
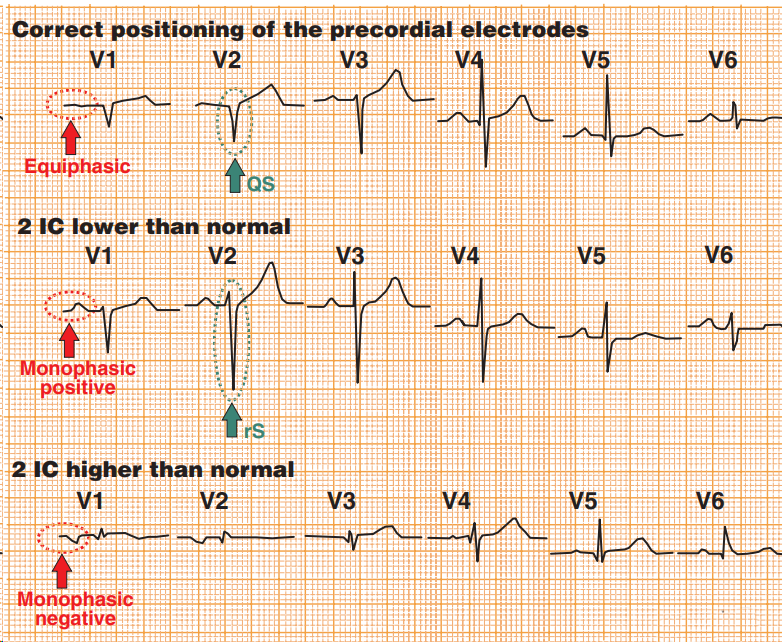
Differential Diagnosis using V1-V2
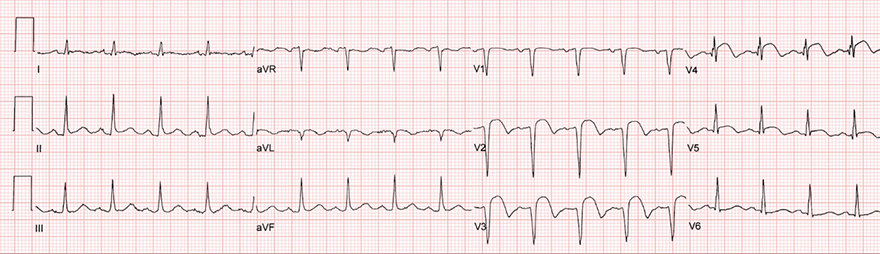
Subacute Anterior STEMI


Old Inferior Wall Infarction

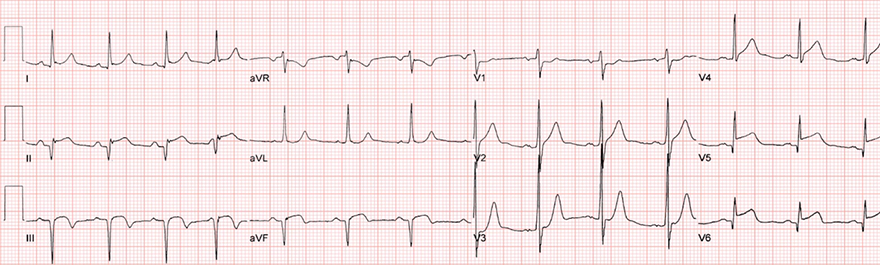
Subacute STEMI of the Inferior and Lateral Walls
Sources
Ischemia Dynamics in Occlusion
|
|
Dynamics of Ischemia After Occlusion
ECG Dynamics of STEMI Infarction
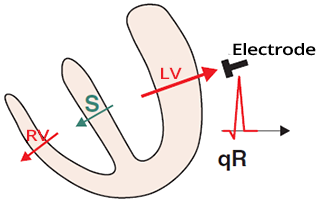
Physiological Q Wave
|
|
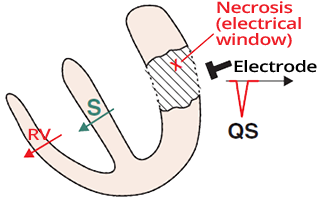
Infarction and Q Wave
|
|
ECG and Post-Infarction Q Wave
|
Old Inferior STEMI
|
|
|
|
Differential Diagnosis using V1-V2
|
|
|
Subacute Anterior STEMI
|
|
|
Old Inferior Wall Infarction
|
|
|
Subacute STEMI of the Inferior and Lateral Walls
|
|
Sources