|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
Upload ECG for Interpretation |
|
|
ECGbook.com Making Medical Education Free for All |
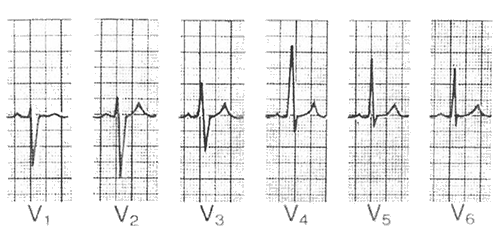
R Wave Progression and Transition Zone
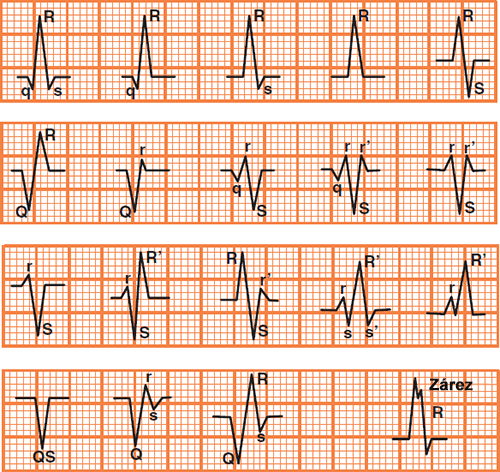
Nomenclature of the QRS Complex
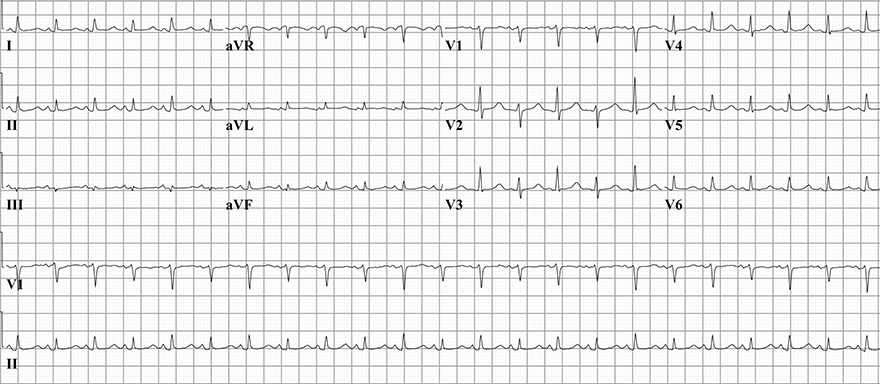
Sinus Rhythm
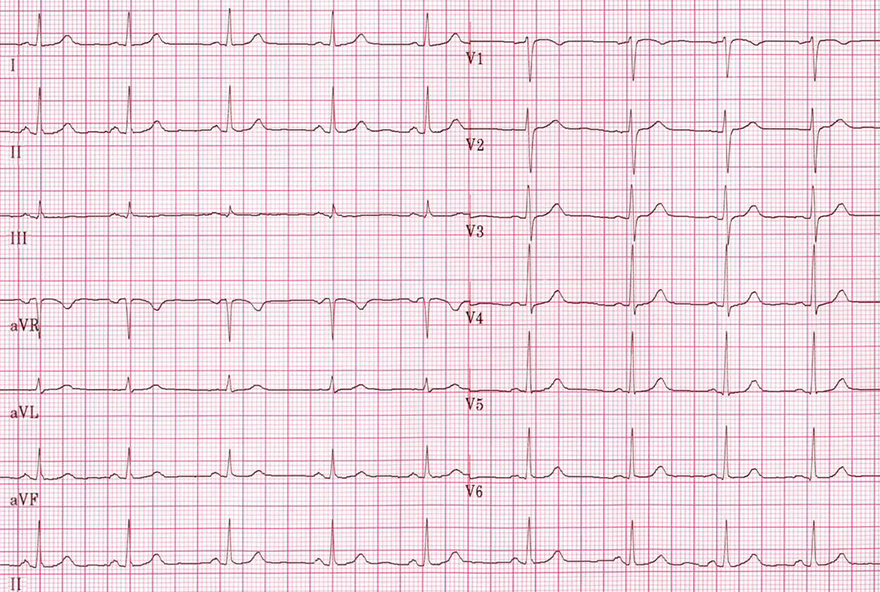
Physiological R Wave
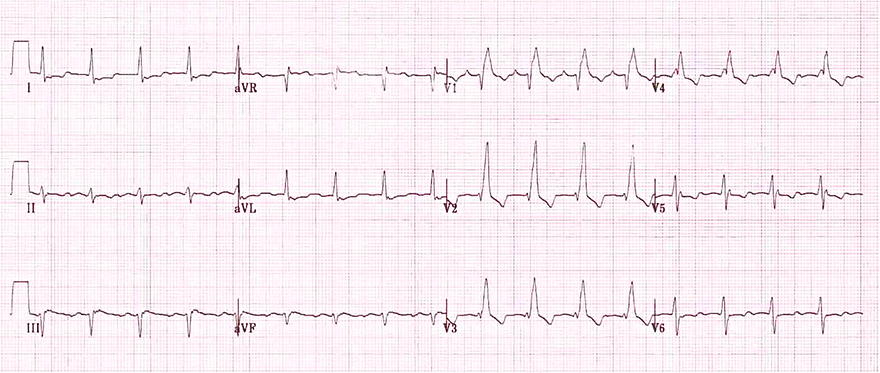
Right Bundle Branch Block
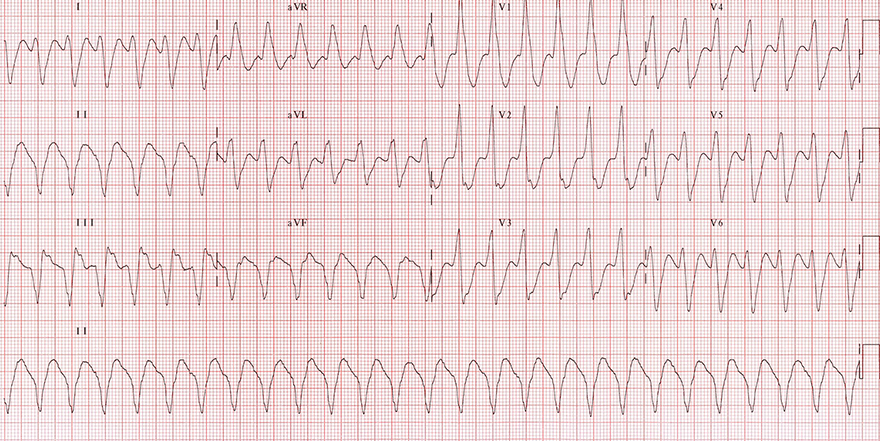
Ventricular Tachycardia
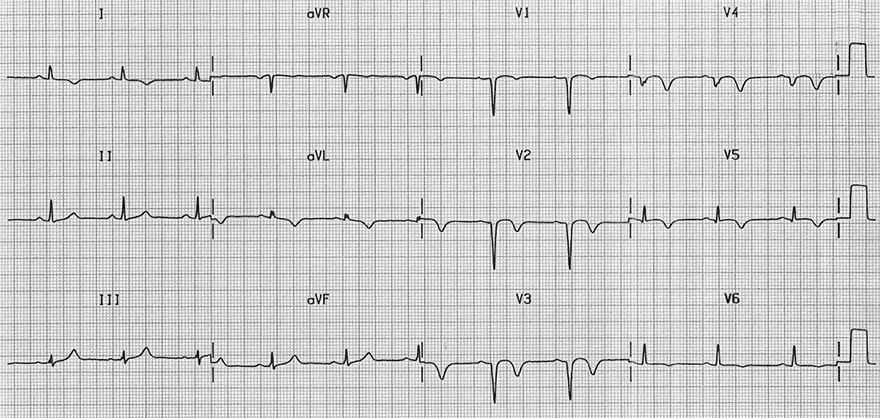
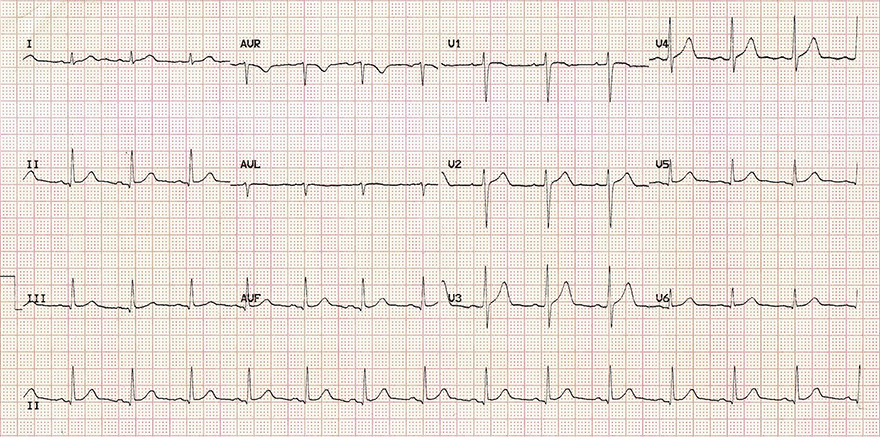
Old Antero-Septal Infarction
Pericardial Effusion
Sources
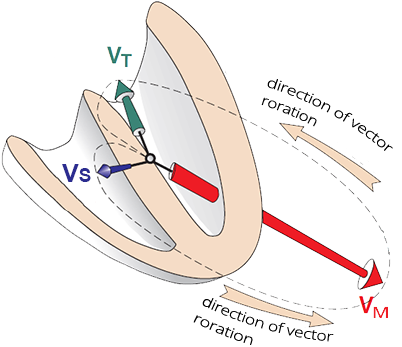
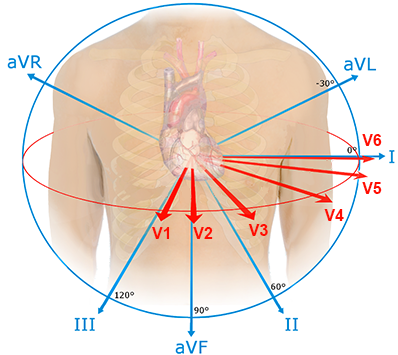
Mechanism of R Wave Formation
|
|
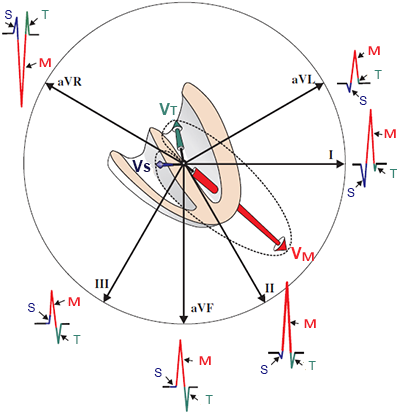
Limb Leads and R Wave
|
|
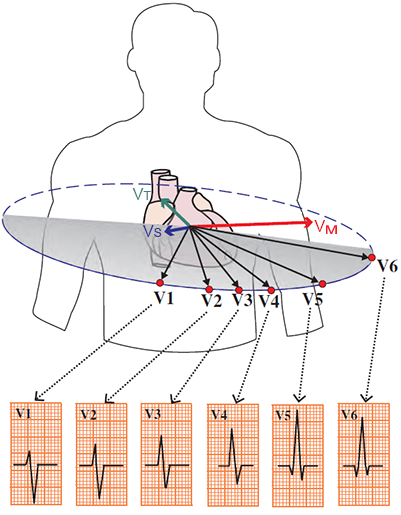
Precordial Leads and R Wave
|
|
|
|
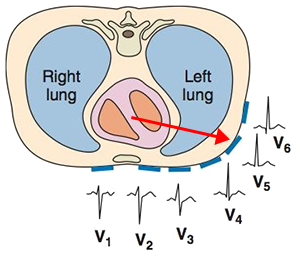
R Wave Progression and Transition Zone
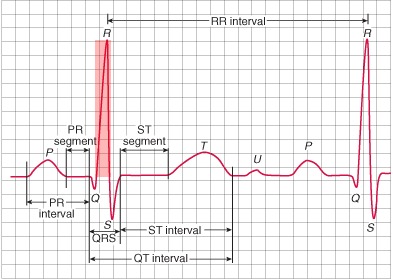
ECG and R Wave
|
|
Nomenclature of the QRS Complex
Pathological R Wave
|
|
Sinus Rhythm
Physiological R Wave
Right Bundle Branch Block
Ventricular Tachycardia
Old Antero-Septal Infarction
Pericardial Effusion
Sources