|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
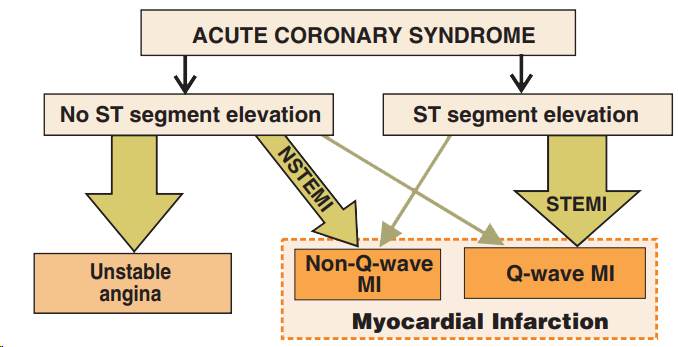
Acute Coronary Syndrome
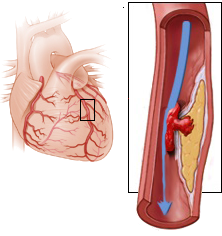
STEMI Infarction

NSTEMI Infarction




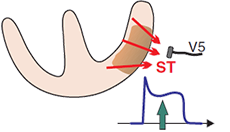
ST Elevations (STE) in STEMI

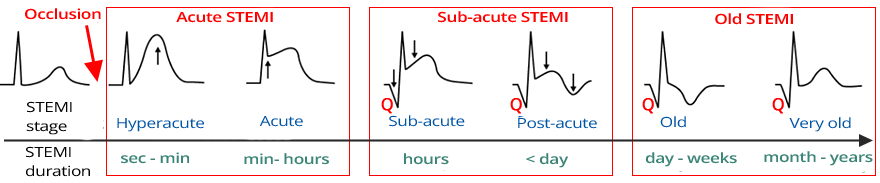
Classification of STEMI by Stage




Reciprocal Changes and Acute Inferior STEMI

| Infarction | ST Elevations | Reciprocal Changes | Occluded Vessel |
| Septal | V1-V2 | LAD | |
| Anterior | V3-V4 (V2, V5) | II, III, aVF | LAD |
| Antero-septal | V1-V4 | II, III, aVF | LAD |
| Lateral | V5-V6 (I, aVL) | II, III, aVF | LCx |
| High Lateral | I, aVL | II, III, aVF | LAD |
| Inferior | II, III, aVF | V2, V3 (I, aVL) | RCA, LCx |
| Posterior | V7-V9 | V1-V3 | RCA, LCA |
| Right Ventricular | V1, V4R | I, aVL | RCA |
| Atrial | Pta (V5, V6, I) | Pta (I, II, III) | RCA |

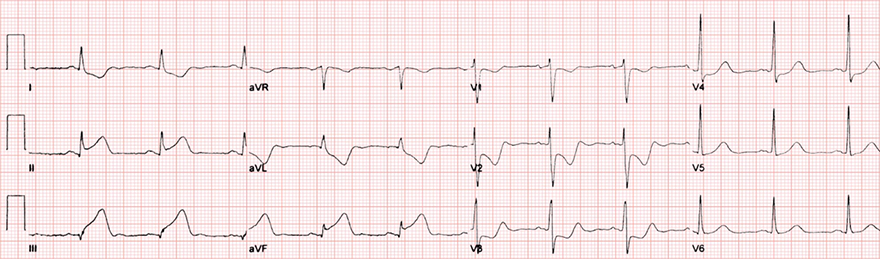
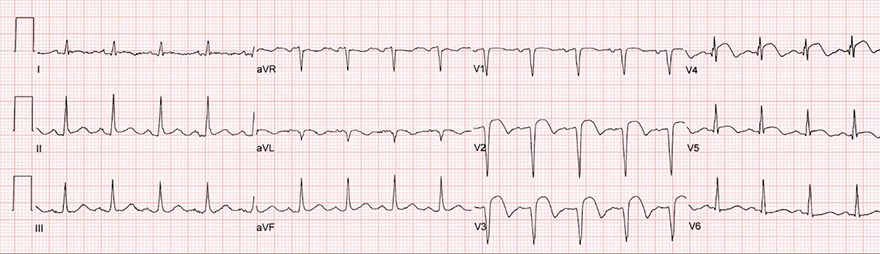
Hyperacute Anterior STEMI
Unstable Angina Pectoris

Pseudonormalization - Hyperacute STEMI

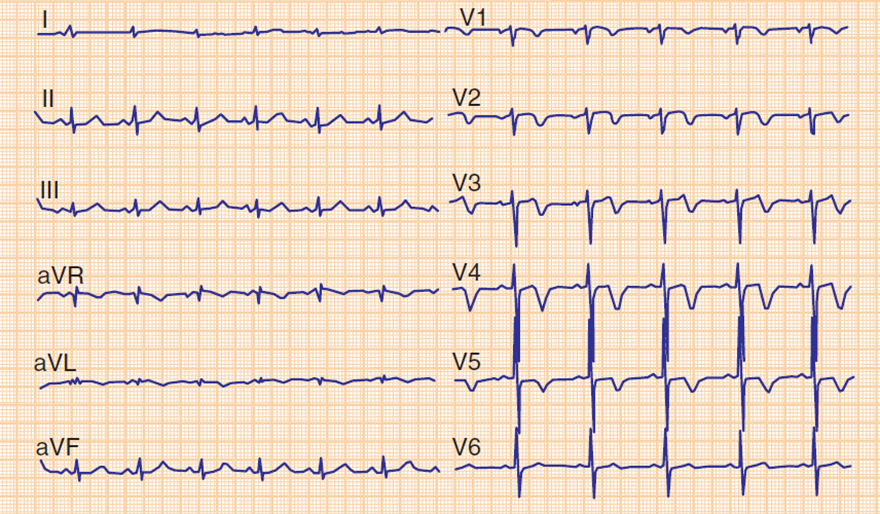
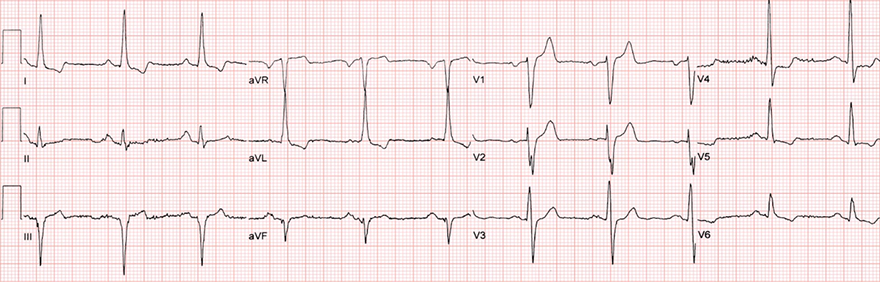
Acute Inferior STEMI
Subacute Anterior STEMI

Old Inferior Wall Infarction

Subacute Inferior and Lateral Wall STEMI
Sources
Acute Coronary Syndrome
Infarct Nomenclature
|
STEMI Infarction
|
NSTEMI Infarction
|
STEMI Infarction
|
|
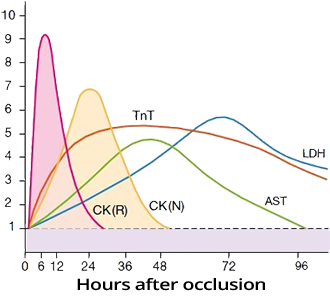
Troponin and Infarction
|
|
|
|
ST Elevations (STE) in STEMI
Pardee Waves
|
|
Classification of STEMI by Stage
|
|
Reciprocal Changes and STEMI
|
|
|
|
|
Reciprocal Changes and Acute Inferior STEMI
STEMI by Location
|
|
| Infarction | ST Elevations | Reciprocal Changes | Occluded Vessel |
| Septal | V1-V2 | LAD | |
| Anterior | V3-V4 (V2, V5) | II, III, aVF | LAD |
| Antero-septal | V1-V4 | II, III, aVF | LAD |
| Lateral | V5-V6 (I, aVL) | II, III, aVF | LCx |
| High Lateral | I, aVL | II, III, aVF | LAD |
| Inferior | II, III, aVF | V2, V3 (I, aVL) | RCA, LCx |
| Posterior | V7-V9 | V1-V3 | RCA, LCA |
| Right Ventricular | V1, V4R | I, aVL | RCA |
| Atrial | Pta (V5, V6, I) | Pta (I, II, III) | RCA |
|
Hyperacute Anterior STEMI
|
|
|
Unstable Angina Pectoris
|
|
|
Pseudonormalization - Hyperacute STEMI
|
|
|
Acute Inferior STEMI
|
|
|
Subacute Anterior STEMI
|
|
|
Old Inferior Wall Infarction
|
|
|
Subacute Inferior and Lateral Wall STEMI
|
|
Sources