|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |
|
|
ECGbook.com Making Medical Education Free for All |

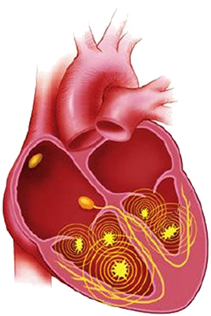
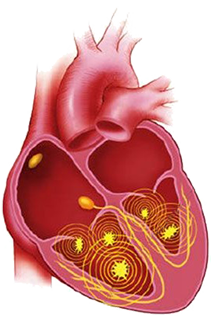
Multiple Micro Re-entries
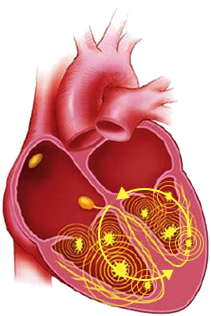
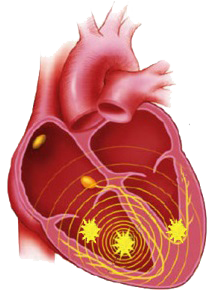
Mother Rotor Re-entry Circuit
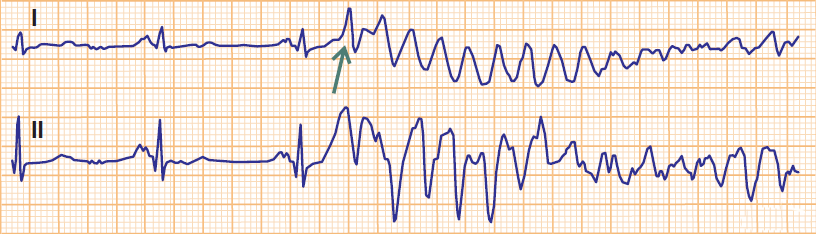
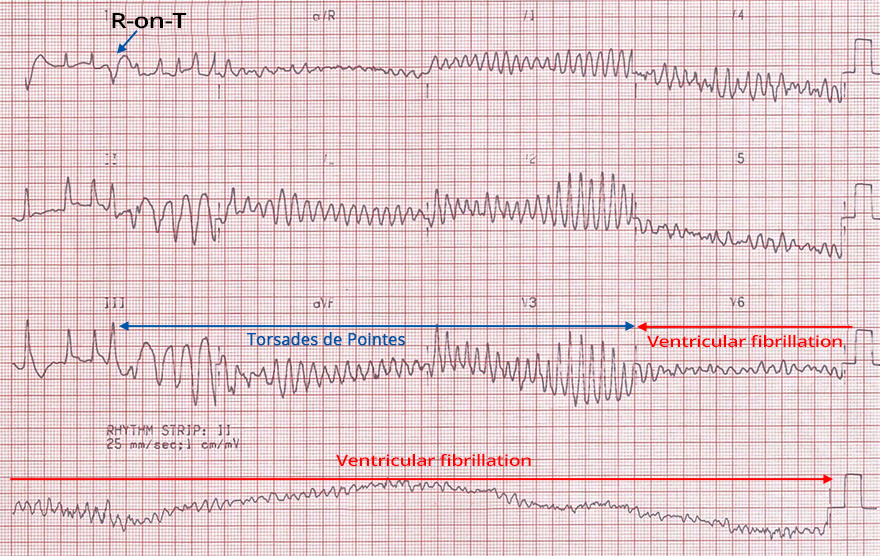
R-on-T Phenomenon and Ventricular Fibrillation

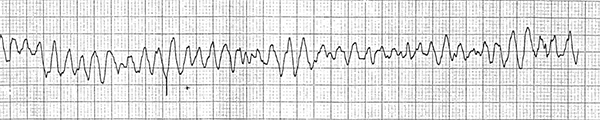
Coarse Ventricular Fibrillation

Fine Ventricular Fibrillation

Fine Ventricular Fibrillation and Asystole
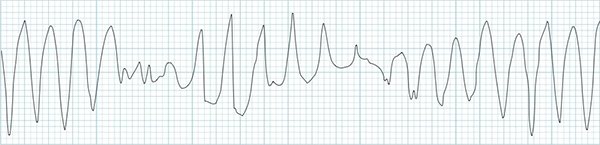
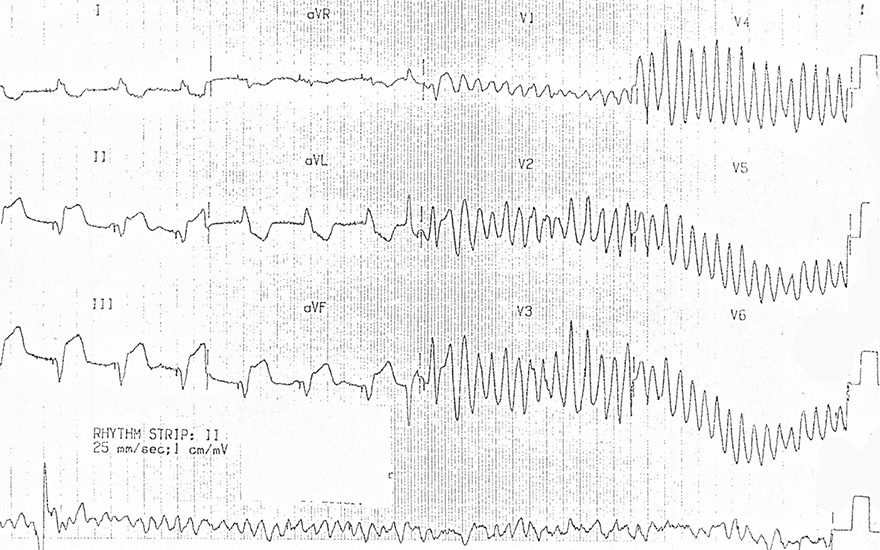
Polymorphic Ventricular Tachycardia
Ventricular Fibrillation





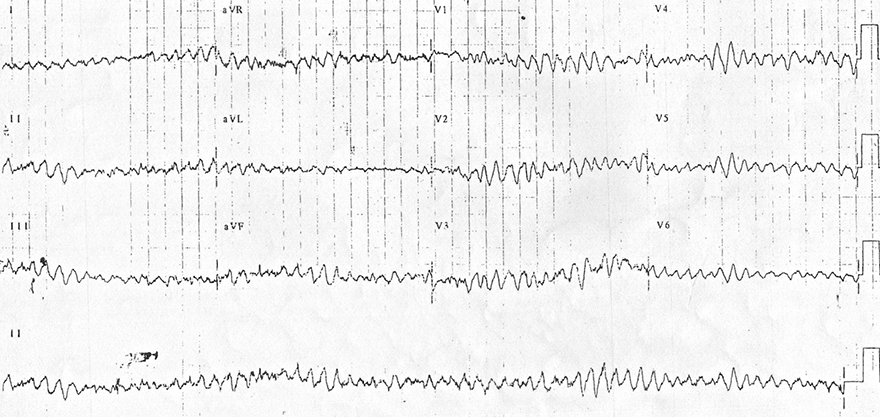
Ventricular Fibrillation
Ventricular Fibrillation
Ventricular Fibrillation

Ventricular Fibrillation and Accelerated Ventricular Rhythm
Sources
Ventricular Fibrillation
|
|
|
|
|
|
Multiple Micro Re-entries
|
Mother Rotor Re-entry Circuit
|
R-on-T Phenomenon and Ventricular Fibrillation
Coarse Ventricular Fibrillation
Fine Ventricular Fibrillation
Fine Ventricular Fibrillation and Asystole
|
|
Polymorphic Ventricular Tachycardia
|
|
|
Ventricular Fibrillation
|
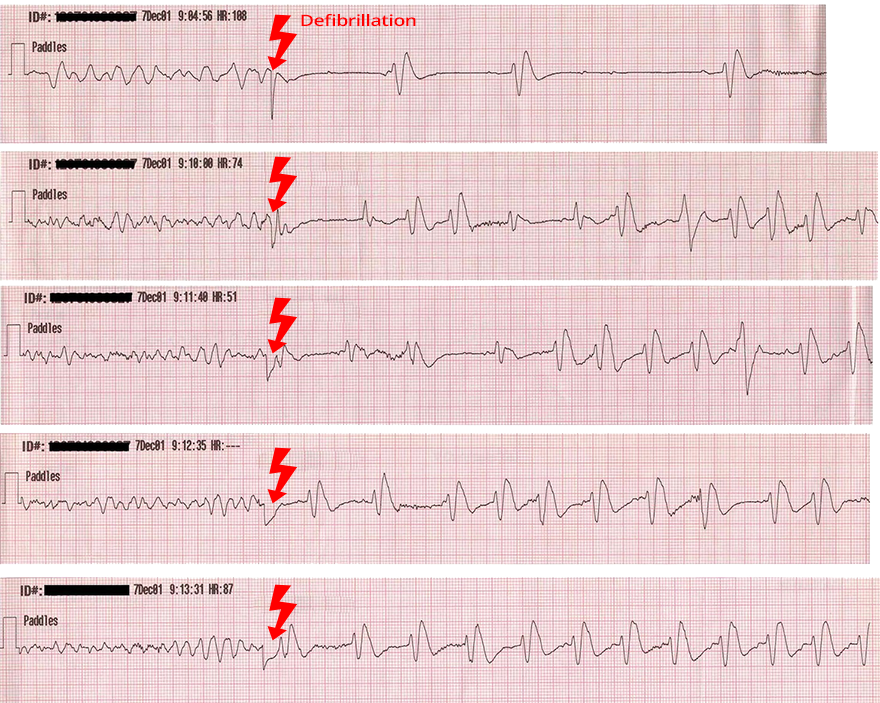
Defibrillator
|
|
|
|
|
Defibrillation
|
|
|
Ventricular Fibrillation
|
|
|
Ventricular Fibrillation
|
|
|
Ventricular Fibrillation
|
|
|
Ventricular Fibrillation and Accelerated Ventricular Rhythm
|
|
Sources